

Factors That Influence Conversion to Resectability and Survival After Resection of Metastases in RAS WT Metastatic Colorectal Cancer (mCRC): Analysis of FIRE-3- AIOKRK0306
- PMID: 32172334
- PMCID: PMC7311511
- DOI: 10.1245/s10434-020-08219-w
Factors That Influence Conversion to Resectability and Survival After Resection of Metastases in RAS WT Metastatic Colorectal Cancer (mCRC): Analysis of FIRE-3- AIOKRK0306
Abstract
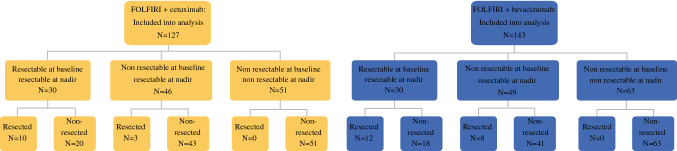
Background: Tumor assessments after first-line therapy of RAS wild-type mCRC with cetuximab (cet) versus bevacizumab (bev) in combination with FOLFIRI were evaluated for factors influencing resectability, conversion to resectability, and survival after best response.
Methods: Conversion to resectability was defined as conversion of initially unresectable to resectable disease at best response as determined by retrospective assessment. Univariate and multivariate logistic models were fitted with resectability at best response as response variable. A Cox model comparing the survival from best response was used to measure the influence of treatment, resectability at best response, and resection. Interaction of resection and treatment arm on survival was tested by likelihood ratio test.
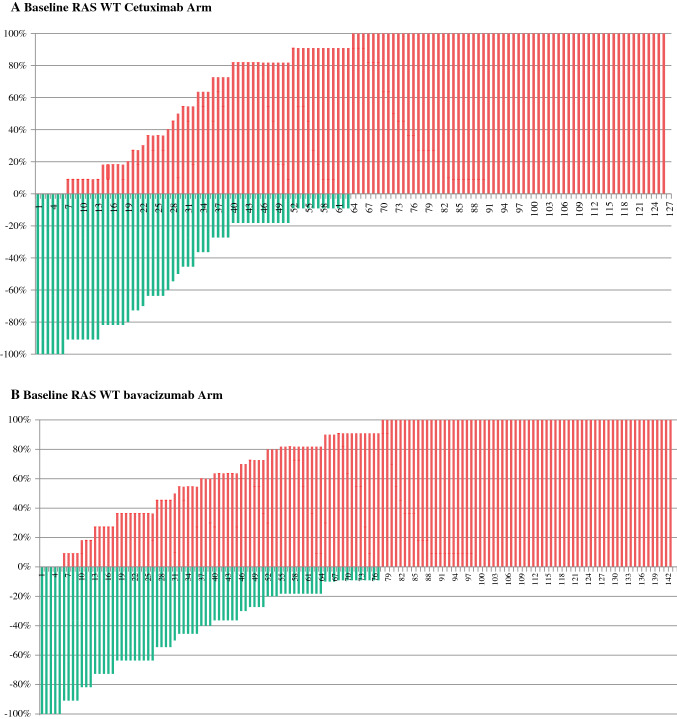
Results: Overall, 270 patients were evaluable (127 cet-arm, 143 bev-arm). Lung metastases (odds ratio [OR] 0.35, 95% confidence response [CI] 0.19-0.63), BRAF mutation (OR 0.33, 95% CI 0.12-0.82), and elevated alkaline phosphatase (OR 0.42, 95% CI 0.18-0.9) before randomization were associated with less chance of successful conversion and were integrated into a nomogram. Early tumor shrinkage (OR 1.86, 95% CI 1.06-3.3; p 0.034) and depth of response (OR 1.02, 95% CI 1.01-1.03; p < 0.001) were associated with successful conversion therapy. Resection of metastases improved post-best-response survival (hazard ratio 0.53, 95% CI 0.29-0.97; p = 0.039), predominantely in cet-treated patients (interaction test, p = 0.02).
Conclusions: Conversion to resectability is significantly associated with baseline characteristics that can be used in a nomogram to predict conversion. Moreover, early efficacy parameters (ETS and DpR) are associated with successful conversion therapy. In FIRE-3, resection of metastases was associated with improved post-best response survival, this effect originated predominantly from the cetuximab-based study arm.
Conflict of interest statement
All other authors reported no potential conflicts of interest.
Figures




References
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Research Materials
