

Association of Serum Lipoprotein (a) With the Requirement for a Peripheral Artery Operation and the Incidence of Major Adverse Cardiovascular Events in People With Peripheral Artery Disease
- PMID: 32172653
- PMCID: PMC7335512
- DOI: 10.1161/JAHA.119.015355
Association of Serum Lipoprotein (a) With the Requirement for a Peripheral Artery Operation and the Incidence of Major Adverse Cardiovascular Events in People With Peripheral Artery Disease
Abstract
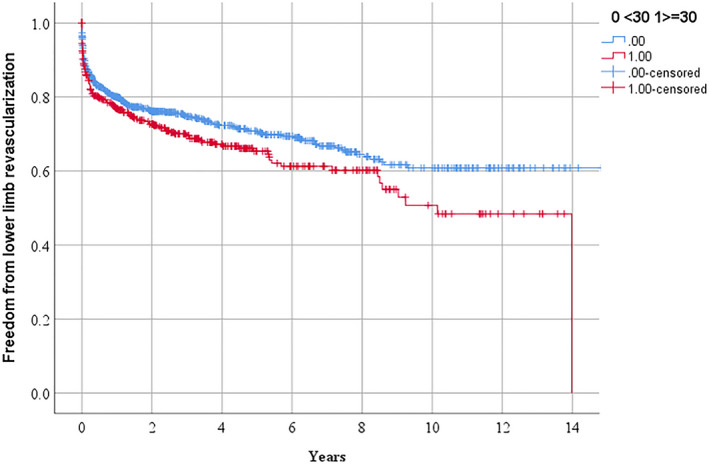
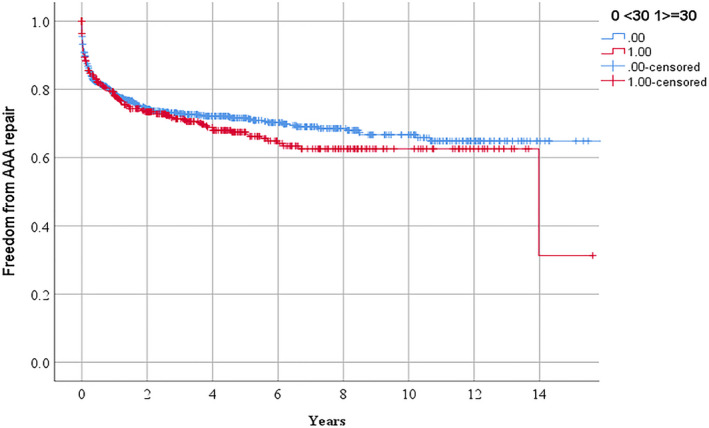
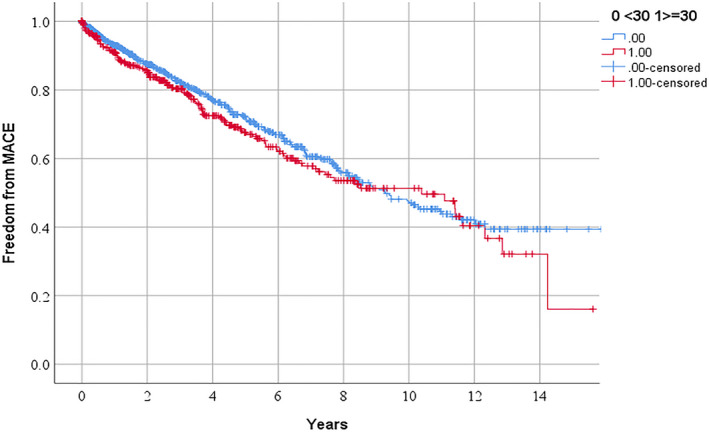
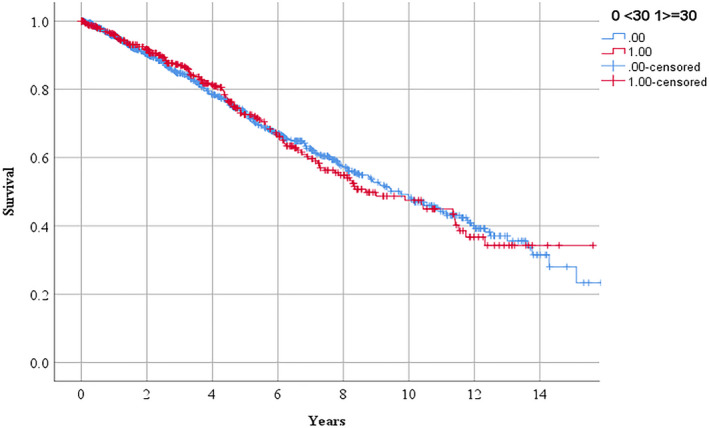
Background The aim of this study was to assess the relationship between serum lipoprotein (a) (Lp[a]) concentration and the requirement for peripheral artery disease (PAD) operations or incidence of major adverse cardiovascular events. Methods and Results A total of 1472 people with PAD presenting with intermittent claudication (n=355), abdominal aortic aneurysm (n=989) or critical limb ischemia (n=128) were prospectively recruited from 4 outpatient clinics in Australia. Lp(a) was measured in serum samples collected at recruitment using an immunoassay. Participants were followed for a median (interquartile range) of 2.4 (0.1-6.1) years to record requirement for any PAD operation, defined to include any open or endovascular PAD intervention (lower limb peripheral revascularization, abdominal aortic aneurysm repair, other aneurysm repair, or carotid artery revascularization). Myocardial infarctions, strokes, and deaths were also recorded. The association of Lp(a) with events was assessed using Cox proportional hazard analysis adjusting for traditional risk factors. Participants with Lp(a) ≥30 mg/dL had a greater requirement for any PAD operation (hazard ratio, 1.20, 95% CI, 1.02-1.41) and lower limb peripheral revascularization alone (hazard ratio 1.33, 95% CI, 1.06-1.66) but no increased risk of major adverse cardiovascular events or all-cause mortality. Lp(a) ≥50 mg/dL and a 40 mg/dL increase in Lp(a) were also associated with an increased risk of lower limb peripheral revascularization alone but not with other outcomes. Conclusions In participants with PAD referred for hospital management those with high Lp(a) had greater requirement for lower limb peripheral revascularization but Lp(a) was not consistently associated with other clinical events.
Keywords: Peripheral artery disease; lipoprotein (a); surgical treatment.
Figures

References
-
- Fowkes FG, Aboyans V, Fowkes FJ, McDermott MM, Sampson UK, Criqui MH. Peripheral artery disease: epidemiology and global perspectives. Nat Rev Cardiol. 2017;14:156–170. - PubMed
-
- Fowkes FG, Rudan D, Rudan I, Aboyans V, Denenberg JO, McDermott MM, Norman PE, Sampson UK, Williams LJ, Mensah GA, et al. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: a systematic review and analysis. Lancet. 2013;382:1329–1340. - PubMed
-
- Sampson UK, Norman PE, Fowkes FG, Aboyans V, Song Y, Harrell FE Jr, Forouzanfar MH, Naghavi M, Denenberg JO, McDermott MM, et al. Estimation of global and regional incidence and prevalence of abdominal aortic aneurysms 1990 to 2010. Glob Heart. 2014;9:159–170. - PubMed
-
- Golledge J. Lower-limb arterial disease. Lancet. 1997;350:1459–1465. - PubMed
-
- Thomas Manapurathe D, Moxon JV, Krishna SM, Rowbotham S, Quigley F, Jenkins J, Bourke M, Bourke B, Jones RE, Golledge J. Cohort study examining the association between blood pressure and cardiovascular events in patients with peripheral artery disease. J Am Heart Assoc. 2019;8:e010748 DOI: 10.1161/JAHA.118.010748. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
