

Feasibility of Venovenous Extracorporeal Membrane Oxygenation Without Systemic Anticoagulation
- PMID: 32173339
- PMCID: PMC7486253
- DOI: 10.1016/j.athoracsur.2020.02.011
Feasibility of Venovenous Extracorporeal Membrane Oxygenation Without Systemic Anticoagulation
Abstract
Background: Venovenous extracorporeal membrane oxygenation (ECMO) is increasingly being used for acute respiratory distress syndrome and as a bridge to lung transplantation. After initiation of venovenous ECMO, systemic anticoagulation therapy is traditionally administered and can cause bleeding diathesis. Here, we investigated whether venovenous ECMO can be administered without continuous systemic anticoagulation administration for patients with acute respiratory distress syndrome.
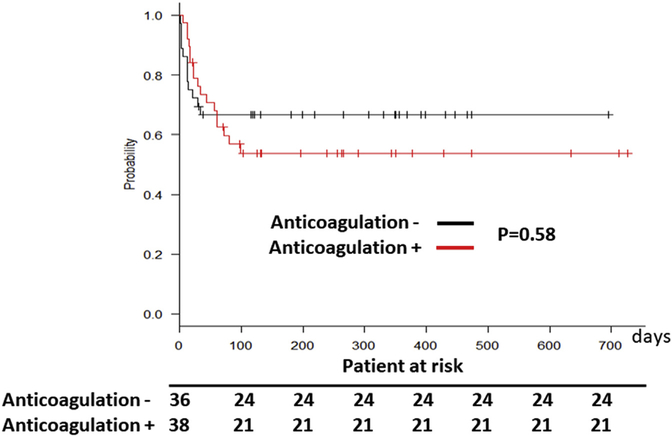
Methods: This is a retrospective review of an institutional ECMO database. We included consecutive patients from January 2015 through February 2019. Overall, 38 patients received low levels of continuous systemic anticoagulation (AC+) whereas the subsequent 36 patients received standard venous thromboprophylaxis (AC-). Published Extracorporeal Life Support Organization guidelines were used for the definition of outcomes and complications.
Results: Overall, survival was not different between the two groups (P = .58). However, patients in the AC+ group had higher rates of gastrointestinal bleeding (28.9%, vs AC- group 5.6%; P < .001). The events per patient-day of gastrointestinal bleeding was 0.00025 in the AC- group and 0.00064 in the AC+ group (P < .001). In addition, oxygenator dysfunction was increased in the AC+ group (28.9% and 0.00067 events per patient-day, vs AC- 11.1% and 0.00062 events per patient-day; P = .02). Furthermore, the AC+ group received more transfusions: packed red blood cells, AC+ group 94.7% vs AC- group 55.5% (P < .001); fresh frozen plasma, AC+ 60.5% vs AC- 16.6% (P = .001); and platelets, AC+ 84.2% vs AC- 27.7% (P < .001). There was no circuit thrombosis in either groups throughout the duration of ECMO support.
Conclusions: Our results suggest that venovenous ECMO can be safely administered without continuous systemic anticoagulation therapy. This approach may be associated with reduced bleeding diathesis and need for blood transfusions.
Copyright © 2020 The Society of Thoracic Surgeons. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Extracorporeal Membrane Oxygenation, Circuits, and Coatings "Pro and Cons" During Anticoagulation.Ann Thorac Surg. 2022 Jan;113(1):374-375. doi: 10.1016/j.athoracsur.2021.02.060. Epub 2021 Mar 8. Ann Thorac Surg. 2022. PMID: 33705775 No abstract available.
-
Modern Extracorporeal Membrane Oxygenation Circuitry May Obviate the Need for Continuous Systemic Anticoagulation.Ann Thorac Surg. 2022 Jan;113(1):375. doi: 10.1016/j.athoracsur.2021.04.073. Epub 2021 May 8. Ann Thorac Surg. 2022. PMID: 33974891 No abstract available.
References
-
- Karagiannidis C, Brodie D, Strassmann S, et al. Extracorporeal membrane oxygenation: evolving epidemiology and mortality. Intensive Care Med. 2016;42:889–896. - PubMed
-
- Lehr CJ, Zaas DW, Cheifetz IM, Turner DA. Ambulatory extracorporeal membrane oxygenation as a bridge to lung transplantation: walking while waiting. Chest. 2015;147:1213–1218. - PubMed
-
- Combes A, Hajage D, Capellier G, et al. Extracorporeal membrane oxygenation for severe acute respiratory distress syndrome. N Engl J Med. 2018;378:1965–1975. - PubMed
-
- Aubron C, McQuilten Z, Bailey M, et al. Low-dose versus therapeutic anticoagulation in patients on extracorporeal membrane oxygenation: a pilot randomized trial. Crit Care Med. 2019;47:e563–e571. - PubMed
-
- Krueger K, Schmutz A, Zieger B, Kalbhenn J. Venovenous extracorporeal membrane oxygenation with prophylactic subcutaneous anticoagulation only: an observational study in more than 60 patients. Artif Organs. 2017;41:186–192. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
