

Impact of the ACOG guideline regarding low-dose aspirin for prevention of superimposed preeclampsia in women with chronic hypertension
- PMID: 32173446
- PMCID: PMC8299295
- DOI: 10.1016/j.ajog.2020.03.004
Impact of the ACOG guideline regarding low-dose aspirin for prevention of superimposed preeclampsia in women with chronic hypertension
Abstract
Background: Patients with chronic hypertension are at increased risk for superimposed preeclampsia. The 2016 American College of Obstetricians and Gynecologists guideline recommended initiating 81 mg of daily aspirin for all pregnant women with chronic hypertension to prevent superimposed preeclampsia.
Objective: (1) To evaluate the rates of implementation of the 2016 American College of Obstetricians and Gynecologists guideline over time; and (2) to evaluate the effectiveness of aspirin for the prevention of superimposed preeclampsia and other adverse maternal and neonatal outcomes in women with chronic hypertension before and after this guideline.
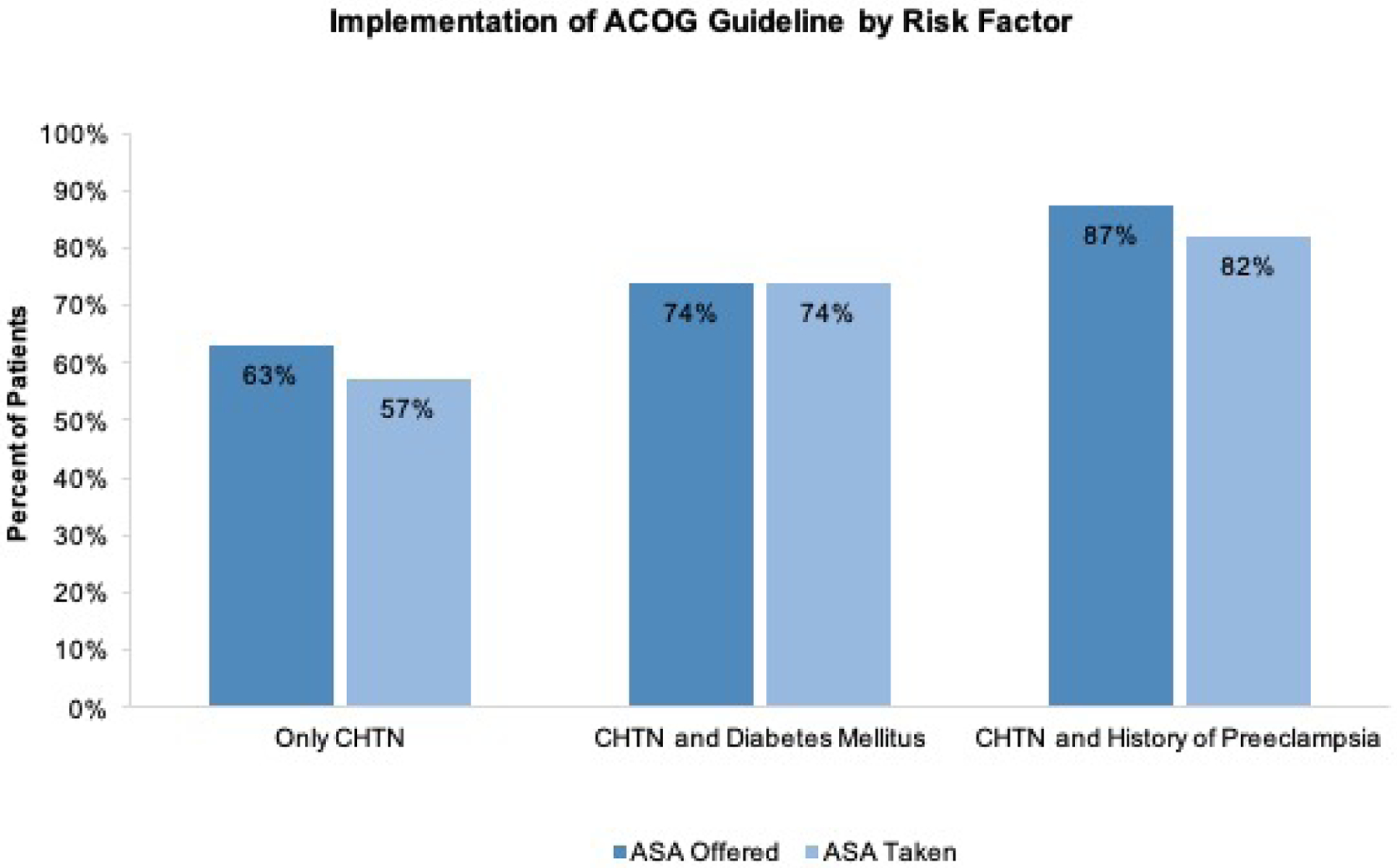
Study design: This is a retrospective study of women with chronic hypertension who delivered at Thomas Jefferson University Hospital from January 2014 through June 2018. This cohort of women with chronic hypertension was divided into 2 groups, before and after the American College of Obstetricians and Gynecologists recommendation published in September 2016. Daily 81 mg of aspirin was initiated between 12 and 16 weeks. We excluded multiple gestations and incomplete records. The primary outcome was incidence of superimposed preeclampsia, and secondary outcomes were incidence of superimposed preeclampsia with or without severe features, small for gestational age, and preterm birth <37 weeks. Subgroup analysis based on risk stratification was evaluated in women with chronic hypertension requiring antihypertensive medication, history of preeclampsia, and pregestational diabetes.
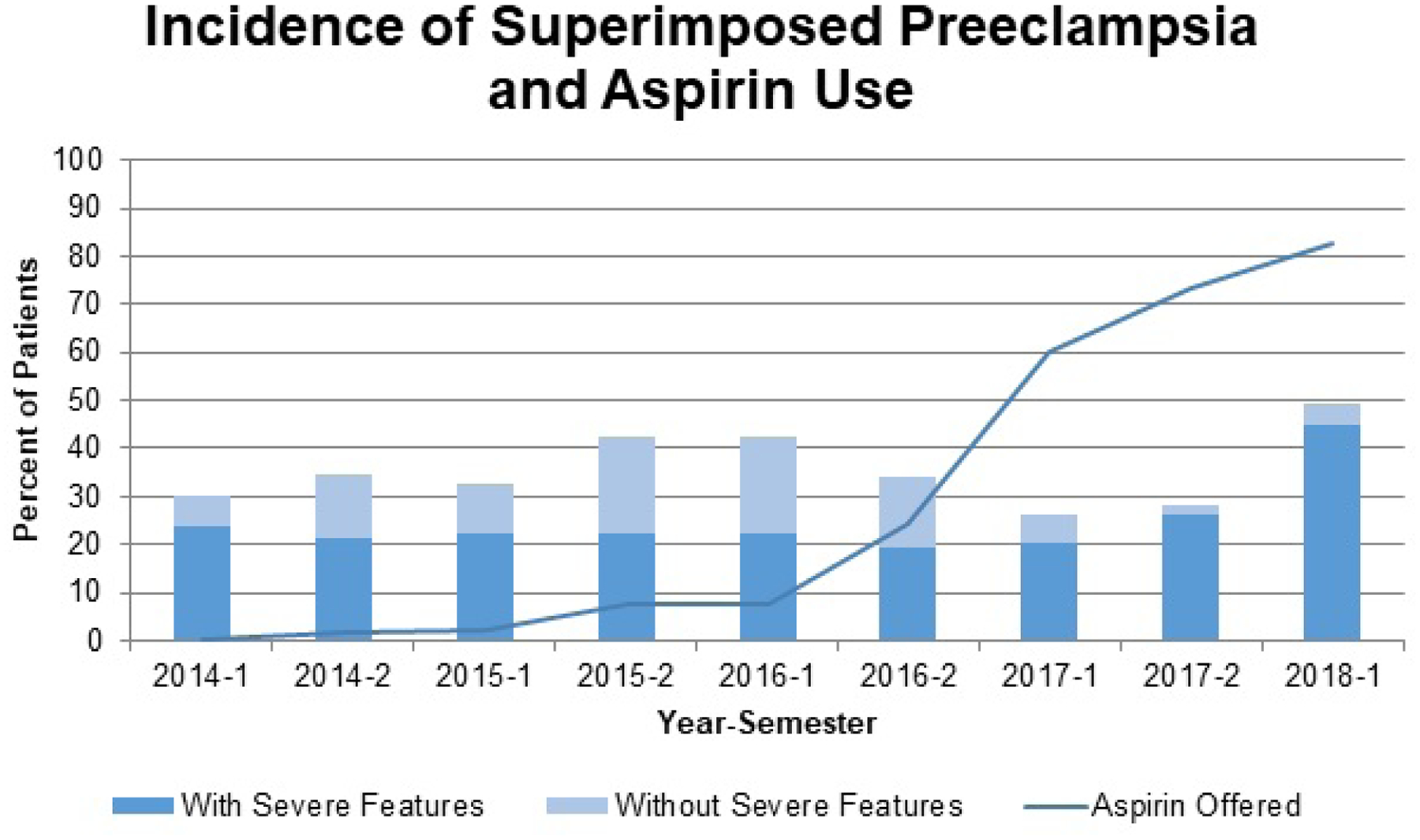
Results: We identified 457 pregnant women with chronic hypertension, 203 in the post-American College of Obstetricians and Gynecologists group and 254 in the pre-American College of Obstetricians and Gynecologists group. Aspirin 81 mg was offered to 142 (70%) in the post-American College of Obstetricians and Gynecologists group and 18 (7.0%) in the pre-American College of Obstetricians and Gynecologists group. Maternal demographics were not significantly different. The overall incidence of superimposed preeclampsia was not significantly different: 87 (34.3%) vs 72 (35.5%), P=.79, in the pre- and post-American College of Obstetricians and Gynecologists guideline groups, respectively. Superimposed preeclampsia with severe features significantly increased: 32 (12.6%) vs 9 (4.4%), P<.01, whereas superimposed preeclampsia without severe features significantly decreased: 55 (21.7%) vs 63 (31.0%), P=.03. There were no significant differences in small for gestational age neonates or preterm birth <37 weeks incidences between groups. There were no significant differences in the subgroup analysis based on the severity of chronic hypertension requiring antihypertensive medication, history of preeclampsia, or pregestational diabetes.
Conclusion: After the adoption of the American College of Obstetricians and Gynecologists guidelines in 70% of the cohort, superimposed preeclampsia, small for gestational age, and preterm birth were not significantly decreased after implementation of aspirin 81 mg initiated between 12 and 16 weeks of gestation.
Keywords: ACOG; aspirin; chronic hypertension; low-dose aspirin; preeclampsia; preterm birth; small for gestational age; superimposed preeclampsia.
Copyright © 2020 Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
81-mg aspirin: a dosing dilemma.Am J Obstet Gynecol. 2021 Apr;224(4):414. doi: 10.1016/j.ajog.2020.12.001. Epub 2020 Dec 8. Am J Obstet Gynecol. 2021. PMID: 33306965 No abstract available.
-
81 mg aspirin: a dosing dilemma response.Am J Obstet Gynecol. 2021 Apr;224(4):414-415. doi: 10.1016/j.ajog.2020.11.038. Epub 2020 Dec 8. Am J Obstet Gynecol. 2021. PMID: 33306966 No abstract available.
-
Impact of aspirin on preeclampsia response.Am J Obstet Gynecol. 2021 May;224(5):545-546. doi: 10.1016/j.ajog.2020.11.036. Epub 2020 Dec 8. Am J Obstet Gynecol. 2021. PMID: 33306969 No abstract available.
-
Impact of aspirin on preeclampsia.Am J Obstet Gynecol. 2021 May;224(5):544-545. doi: 10.1016/j.ajog.2020.12.004. Epub 2020 Dec 8. Am J Obstet Gynecol. 2021. PMID: 33306972 No abstract available.
References
-
- WHO Recommendations for Prevention and Treatment of Pre-Eclampsia and Eclampsia. Geneva; 2011. - PubMed
-
- Say L, Chou D, Gemmill A, et al. Global causes of maternal death: a WHO systematic analysis. The Lancet Global health 2014; 2(6): e323–33. - PubMed
-
- American College of O, Gynecologists, Task Force on Hypertension in P. Hypertension in pregnancy. Report of the American College of Obstetricians and Gynecologists’ Task Force on Hypertension in Pregnancy. Obstet Gynecol 2013; 122(5): 1122–31. - PubMed
-
- Burton GJ, Redman CW, Roberts JM, Moffett A. Pre-eclampsia: pathophysiology and clinical implications. Bmj 2019; 366: l2381. - PubMed
-
- Dekker GA, Sibai BM. Etiology and pathogenesis of preeclampsia: current concepts. Am J Obstet Gynecol 1998; 179(5): 1359–75. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
