

Fracture risk following high-trauma versus low-trauma fracture: a registry-based cohort study
- PMID: 32173782
- PMCID: PMC7115893
- DOI: 10.1007/s00198-019-05274-2
Fracture risk following high-trauma versus low-trauma fracture: a registry-based cohort study
Abstract
Prior high-trauma fractures identified through health services data are associated with low bone mineral density (BMD) and future fracture risk to the same extent as fractures without high-trauma.
Introduction: Some have questioned the usefulness of distinguishing high-trauma fractures from low-trauma fractures. The aim of this study is to compare BMD measurements and risk of subsequent low-trauma fracture in patients with prior high- or low-trauma fractures.
Methods: Using a clinical BMD registry for the province of Manitoba, Canada, we identified women and men age 40 years or older with fracture records from linked population-based healthcare data. Age- and sex-adjusted BMD Z-scores and covariate-adjusted hazard ratios (HR) with 95% confidence intervals (CI) for incident fracture were studied in relation to prior fracture status, categorized as high-trauma if associated with external injury codes and low-trauma otherwise.
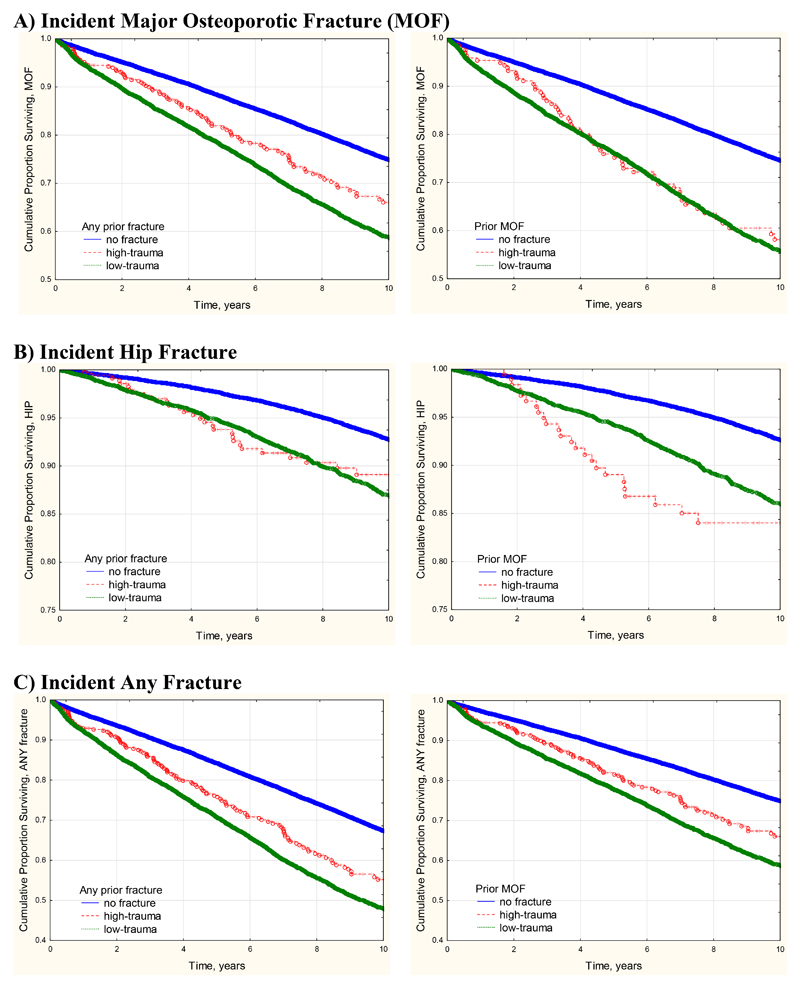
Results: The study population consisted of 64,428 women and men with no prior fracture (mean age 63.7 years), 858 with prior high-trauma fractures (mean age 65.1 years), and 14,758 with prior low-trauma fractures (mean age 67.2 years). Mean Z-scores for those with any prior high-trauma fracture were significantly lower than in those without prior fracture (P < 0.001) and similar to those with prior low-trauma fracture. Median observation time for incident fractures was 8.8 years (total 729,069 person-years). Any prior high-trauma fracture was significantly associated with increased risk for incident major osteoporotic fracture (MOF) (adjusted HR 1.31, 95% CI 1.08-1.59) as was prior low-trauma fracture (adjusted HR 1.55, 95% CI 1.47-1.63), and there was no significant difference between the two groups (prior trauma versus low-trauma fracture P = 0.093). A similar pattern was seen when incident MOF was studied in relation to prior hip fracture or prior MOF, or when the outcome was incident hip fracture or any incident fracture.
Conclusions: High-trauma and low-trauma fractures showed similar relationships with low BMD and future fracture risk. This supports the inclusion of high-trauma fractures in clinical assessment for underlying osteoporosis and in the evaluation for intervention to reduce future fracture risk.
Keywords: Dual-energy X-ray absorptiometry; Fractures; Osteoporosis; Trauma.
Conflict of interest statement
Figures
Comment in
-
Stop (mis)classifying fractures as high- or low-trauma or as fragility fractures.Osteoporos Int. 2020 Jun;31(6):1023-1024. doi: 10.1007/s00198-020-05325-z. Epub 2020 Mar 16. Osteoporos Int. 2020. PMID: 32173783 No abstract available.
References
-
- Compston JE, McClung MR, Leslie WD. Osteoporosis. The Lancet. 2019;393(10169):364–76. - PubMed
-
- Qaseem A, Snow V, Shekelle P, Hopkins R, Jr, Forciea MA, Owens DK, et al. Pharmacologic treatment of low bone density or osteoporosis to prevent fractures: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2008;149(6):404–15. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
