

Low-Attenuation Noncalcified Plaque on Coronary Computed Tomography Angiography Predicts Myocardial Infarction: Results From the Multicenter SCOT-HEART Trial (Scottish Computed Tomography of the HEART)
- PMID: 32174130
- PMCID: PMC7195857
- DOI: 10.1161/CIRCULATIONAHA.119.044720
Low-Attenuation Noncalcified Plaque on Coronary Computed Tomography Angiography Predicts Myocardial Infarction: Results From the Multicenter SCOT-HEART Trial (Scottish Computed Tomography of the HEART)
Abstract
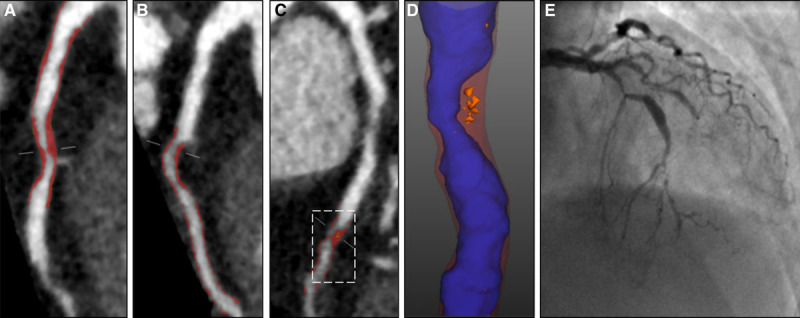
Background: The future risk of myocardial infarction is commonly assessed using cardiovascular risk scores, coronary artery calcium score, or coronary artery stenosis severity. We assessed whether noncalcified low-attenuation plaque burden on coronary CT angiography (CCTA) might be a better predictor of the future risk of myocardial infarction.
Methods: In a post hoc analysis of a multicenter randomized controlled trial of CCTA in patients with stable chest pain, we investigated the association between the future risk of fatal or nonfatal myocardial infarction and low-attenuation plaque burden (% plaque to vessel volume), cardiovascular risk score, coronary artery calcium score or obstructive coronary artery stenoses.
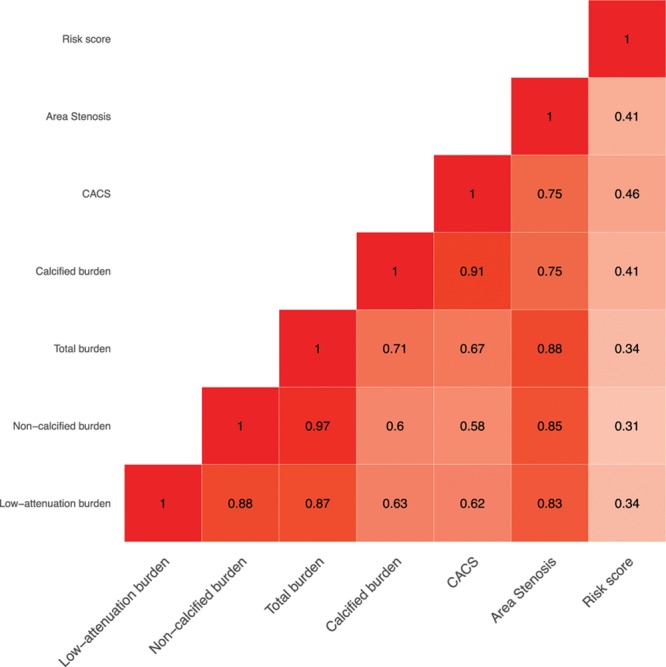
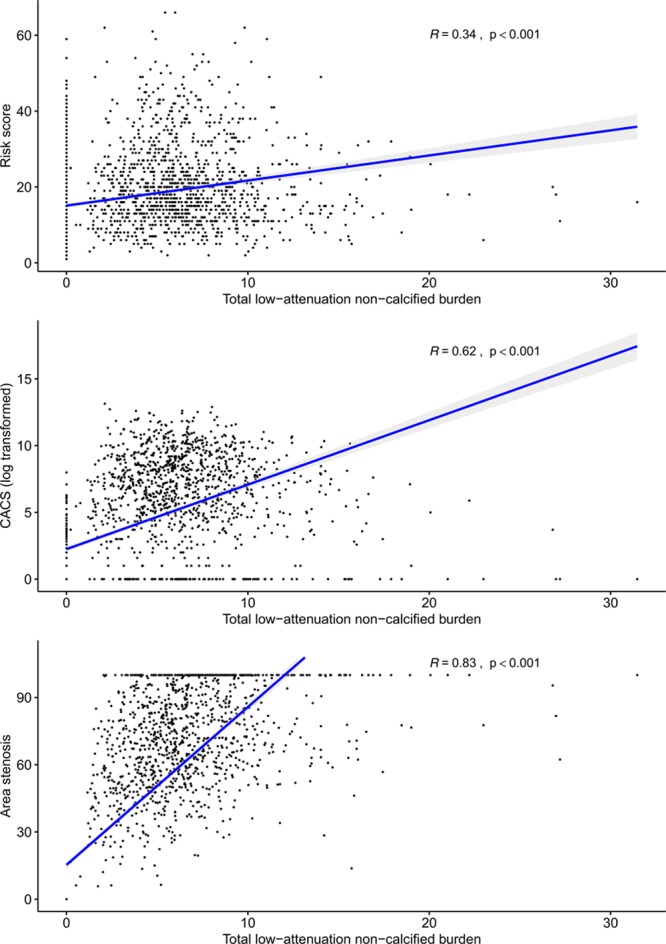
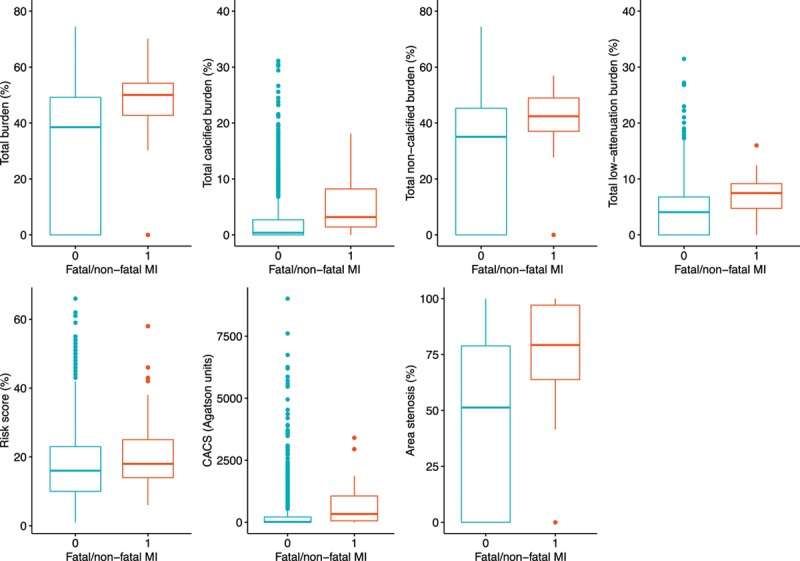
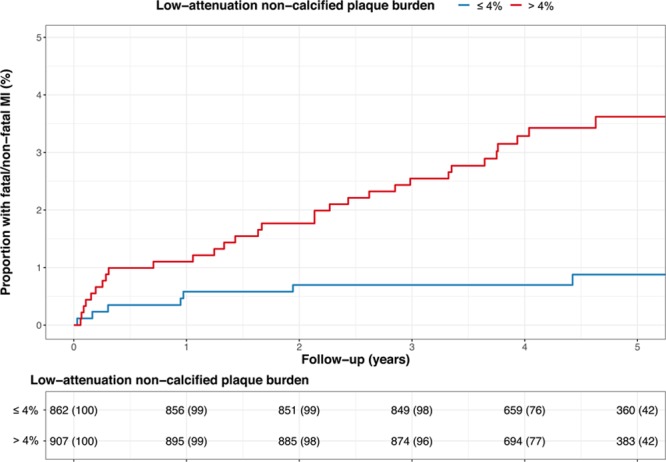
Results: In 1769 patients (56% male; 58±10 years) followed up for a median 4.7 (interquartile interval, 4.0-5.7) years, low-attenuation plaque burden correlated weakly with cardiovascular risk score (r=0.34; P<0.001), strongly with coronary artery calcium score (r=0.62; P<0.001), and very strongly with the severity of luminal coronary stenosis (area stenosis, r=0.83; P<0.001). Low-attenuation plaque burden (7.5% [4.8-9.2] versus 4.1% [0-6.8]; P<0.001), coronary artery calcium score (336 [62-1064] versus 19 [0-217] Agatston units; P<0.001), and the presence of obstructive coronary artery disease (54% versus 25%; P<0.001) were all higher in the 41 patients who had fatal or nonfatal myocardial infarction. Low-attenuation plaque burden was the strongest predictor of myocardial infarction (adjusted hazard ratio, 1.60 (95% CI, 1.10-2.34) per doubling; P=0.014), irrespective of cardiovascular risk score, coronary artery calcium score, or coronary artery area stenosis. Patients with low-attenuation plaque burden greater than 4% were nearly 5 times more likely to have subsequent myocardial infarction (hazard ratio, 4.65; 95% CI, 2.06-10.5; P<0.001).
Conclusions: In patients presenting with stable chest pain, low-attenuation plaque burden is the strongest predictor of fatal or nonfatal myocardial infarction. These findings challenge the current perception of the supremacy of current classical risk predictors for myocardial infarction, including stenosis severity. Registration: URL: https://www.clinicaltrials.gov; Unique identifier: NCT01149590.
Keywords: atherosclerosis; cardiovascular diseases; computed tomography angiography; coronary artery disease; myocardial infarction; plaque, atherosclerotic.
Figures
Comment in
-
Letter by Siontis and Räber Regarding Article, "Low-Attenuation Noncalcified Plaque on Coronary Computed Tomography Angiography Predicts Myocardial Infarction: Results From the Multicenter SCOT-HEART Trial (Scottish Computed Tomography of the HEART)".Circulation. 2020 Oct 20;142(16):e240-e241. doi: 10.1161/CIRCULATIONAHA.120.047472. Epub 2020 Oct 19. Circulation. 2020. PMID: 33074755 No abstract available.
-
Letter by Alfonso et al Regarding Article, "Low-Attenuation Noncalcified Plaque on Coronary Computed Tomography Angiography Predicts Myocardial Infarction: Results From the Multicenter SCOT-HEART Trial (Scottish Computed Tomography of the Heart)".Circulation. 2020 Oct 20;142(16):e242-e243. doi: 10.1161/CIRCULATIONAHA.120.047361. Epub 2020 Oct 19. Circulation. 2020. PMID: 33074756 No abstract available.
-
Response by Williams et al to Letter Regarding Article, "Low-Attenuation Noncalcified Plaque on Coronary Computed Tomography Angiography Predicts Myocardial Infarction: Results From the Multicenter SCOT-HEART Trial (Scottish Computed Tomography of the HEART)".Circulation. 2020 Oct 20;142(16):e244-e245. doi: 10.1161/CIRCULATIONAHA.120.049840. Epub 2020 Oct 19. Circulation. 2020. PMID: 33074760 No abstract available.
References
-
- Knuuti J, Wijns W, Saraste A, Capodanno D, Barbato E, Funck-Brentano C, Prescott E, Storey RF, Deaton C, Cuisset T, et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes: the Task Force for the diagnosis and management of chronic coronary syndromes of the European Society of Cardiology (ESC). European Heart Journal. 2019 doi: 10.1093/eurheartj/ehz425. - DOI
-
- Fihn SD, Blankenship JC, Alexander KP, Bittl JA, Byrne JG, Fletcher BJ, Fonarow GC, Lange RA, Levine GN, Maddox TM, et al. 2014 ACC/AHA/AATS/PCNA/SCAI/STS focused update of the guideline for the diagnosis and management of patients with stable ischemic heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines, and the American Association for Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. Circulation. 2014;130:1749–1767. doi: 10.1161/CIR.0000000000000095. - PubMed
-
- Miller JM, Rochitte CE, Dewey M, Arbab-Zadeh A, Niinuma H, Gottlieb I, Paul N, Clouse ME, Shapiro EP, Hoe J, et al. Diagnostic performance of coronary angiography by 64-row CT. N Engl J Med. 2008;359:2324–2336. doi: 10.1056/NEJMoa0806576. - PubMed
-
- Motoyama S, Sarai M, Harigaya H, Anno H, Inoue K, Hara T, Naruse H, Ishii J, Hishida H, Wong ND, et al. Computed tomographic angiography characteristics of atherosclerotic plaques subsequently resulting in acute coronary syndrome. J Am Coll Cardiol. 2009;54:49–57. doi: 10.1016/j.jacc.2009.02.068. - PubMed
-
- Min JK, Shaw LJ, Devereux RB, Okin PM, Weinsaft JW, Russo DJ, Lippolis NJ, Berman DS, Callister TQ. Prognostic value of multidetector coronary computed tomographic angiography for prediction of all-cause mortality. J Am Coll Cardiol. 2007;50:1161–1170. doi: 10.1016/j.jacc.2007.03.067. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
