

Clinical and Neuropsychological Predictors of Methylphenidate Response in Children and Adolescents with ADHD: A Naturalistic Follow-up Study in a Spanish Sample
- PMID: 32174998
- PMCID: PMC7040471
- DOI: 10.2174/1745017901915010160
Clinical and Neuropsychological Predictors of Methylphenidate Response in Children and Adolescents with ADHD: A Naturalistic Follow-up Study in a Spanish Sample
Abstract
Background: Methylphenidate (MPH) is the most commonly used medication for Attention-Deficit/Hyperactivity Disorder (ADHD), but to date, there are neither consistent nor sufficient findings on conditions differentiating responsiveness to MPH response in ADHD.
Objective: To develop a predictive model of MPH response, using a longitudinal and naturalistic follow-up study, in a Spanish sample of children and adolescents with ADHD.
Methods: We included all children and adolescents with ADHD treated with MPH in our outpatient Clinic (2005 to 2015), evaluated with the K-SADS interview. We collected ADHD-RS-IV.es and CGI-S scores at baseline and at follow up, and neuropsychological testing (WISC-IV, Continuous Performance Test (CPT-II) & Stroop). Clinical response was defined as >30% reduction from baseline of total ADHD-RS-IV.es score and CGI-S final score of 1 or 2 maintained for the previous 3 months.
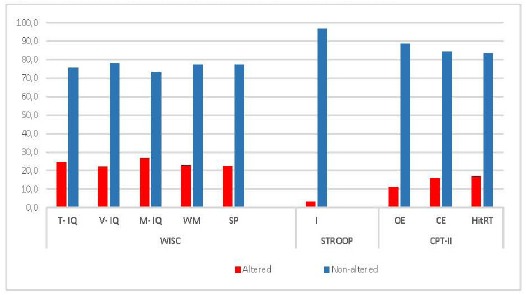
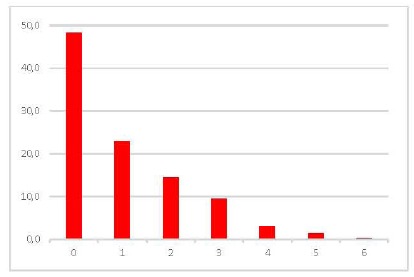
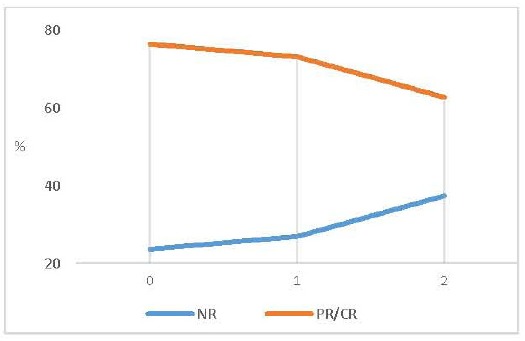
Results: We included 518 children and adolescents with ADHD, mean (SD) age of patients was 11.4 (3.3) years old; 79% male; 51.7% had no comorbidities; and 75.31% had clinical response to a mean MPH dose of 1.2 mg/kg/day. Lower ADHD-RS-IV.es scores, absence of comorbidities (oppositional-defiant symptoms, depressive symptoms and alcohol/cannabis use), fewer altered neuropsychological tests, higher total IQ and low commission errors in CPT-II, were significantly associated with a complete clinical response to methylphenidate treatment.
Conclusion: Oppositional-defiant symptoms, depressive symptoms, and a higher number of impaired neuropsychological tests are associated with worse clinical response to methylphenidate. Other stimulants or non-stimulants treatment may be considered when these clinical and neuropsychological variables converged in the first clinical interview.
Keywords: ADHD; Methylphenidate; Neuropsychological variables; Predictive factors; Spanish sample; Treatment.
© 2019 Bentham Science Publishers.
Figures
Similar articles
-
A post hoc comparison of the effects of lisdexamfetamine dimesylate and osmotic-release oral system methylphenidate on symptoms of attention-deficit hyperactivity disorder in children and adolescents.CNS Drugs. 2013 Sep;27(9):743-51. doi: 10.1007/s40263-013-0086-6. CNS Drugs. 2013. PMID: 23801529 Free PMC article. Clinical Trial.
-
Randomized, Double-Blind, Placebo-Controlled Acute Comparator Trials of Lisdexamfetamine and Extended-Release Methylphenidate in Adolescents With Attention-Deficit/Hyperactivity Disorder.CNS Drugs. 2017 Nov;31(11):999-1014. doi: 10.1007/s40263-017-0468-2. CNS Drugs. 2017. PMID: 28980198 Free PMC article.
-
High pretreatment cognitive impulsivity predicts response of oppositional symptoms to methylphenidate in patients with attention-deficit hyperactivity disorder/oppositional defiant disorder.Int Clin Psychopharmacol. 2019 May;34(3):138-142. doi: 10.1097/YIC.0000000000000252. Int Clin Psychopharmacol. 2019. PMID: 30640748
-
Efficacy of Methylphenidate Hydrochloride Extended-Release Capsules (Aptensio XR™) in Children and Adolescents with Attention-Deficit/Hyperactivity Disorder: A Phase III, Randomized, Double-Blind Study.CNS Drugs. 2015 Apr;29(4):331-40. doi: 10.1007/s40263-015-0241-3. CNS Drugs. 2015. PMID: 25877989 Free PMC article. Clinical Trial.
-
[Atomoxetine: a new treatment for Attention Deficit/Hyperactivity Disorder (ADHD) in children and adolescents].Encephale. 2005 May-Jun;31(3):337-48. doi: 10.1016/s0013-7006(05)82399-1. Encephale. 2005. PMID: 16142049 Review. French.
Cited by
-
Disentangling the Association between ADHD and Alcohol Use Disorder in Individuals Suffering from Bipolar Disorder: A Systematic Review and Meta-Analysis.Brain Sci. 2021 Dec 28;12(1):38. doi: 10.3390/brainsci12010038. Brain Sci. 2021. PMID: 35053783 Free PMC article. Review.
-
Poor response to methylphenidate is associated with a smaller dorsal attentive network in adult Attention-Deficit/Hyperactivity Disorder (ADHD).Transl Psychiatry. 2023 Sep 30;13(1):303. doi: 10.1038/s41398-023-02598-w. Transl Psychiatry. 2023. PMID: 37777529 Free PMC article.
-
Comparing the Effect of Methylphenidate and Anodal tDCS on Inhibitory Control and Working-Memory in Children and Adolescents with Attention Deficit/Hyperactivity Disorder: A Study Protocol for a Randomized, within-Subject Trial.Int J Environ Res Public Health. 2022 Apr 11;19(8):4575. doi: 10.3390/ijerph19084575. Int J Environ Res Public Health. 2022. PMID: 35457447 Free PMC article.
-
Electrophysiological and Clinical Predictors of Methylphenidate, Guanfacine, and Combined Treatment Outcomes in Children With Attention-Deficit/Hyperactivity Disorder.J Am Acad Child Adolesc Psychiatry. 2023 Apr;62(4):415-426. doi: 10.1016/j.jaac.2022.08.001. Epub 2022 Aug 10. J Am Acad Child Adolesc Psychiatry. 2023. PMID: 35963559 Free PMC article. Clinical Trial.
-
Moderators and Other Predictors of Methylphenidate Response in Children and Adolescents with ADHD.Int J Environ Res Public Health. 2022 Jan 31;19(3):1640. doi: 10.3390/ijerph19031640. Int J Environ Res Public Health. 2022. PMID: 35162663 Free PMC article.
References
-
- American Psychiatric Association (APA) Diagnostic and statistical manual of mental disorders. 2013.
LinkOut - more resources
Full Text Sources