

Acute scaphoid fractures: guidelines for diagnosis and treatment
- PMID: 32175096
- PMCID: PMC7047900
- DOI: 10.1302/2058-5241.5.190025
Acute scaphoid fractures: guidelines for diagnosis and treatment
Abstract
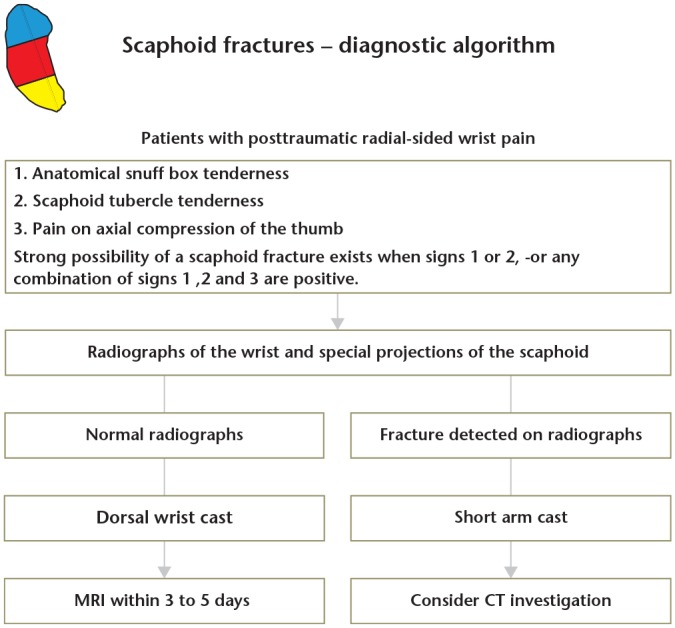
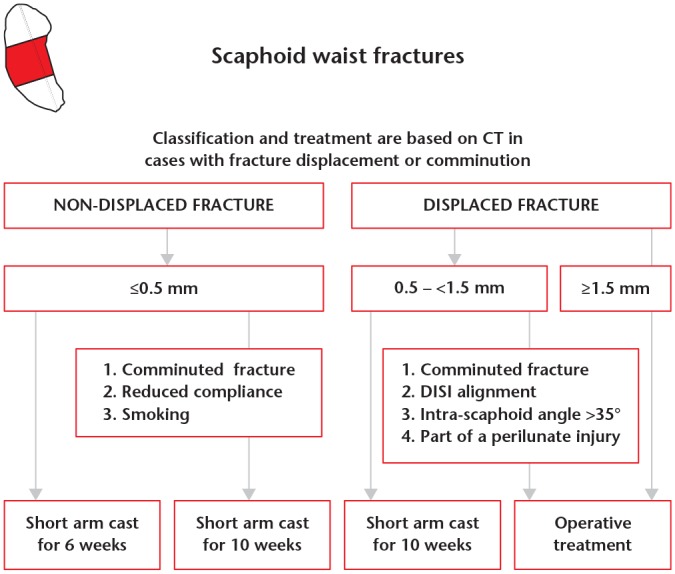
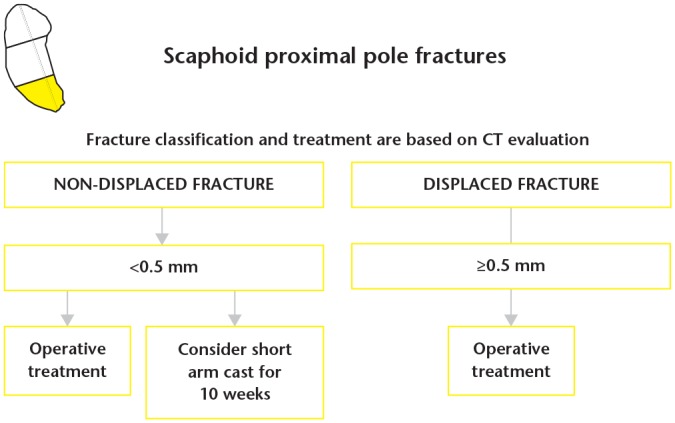
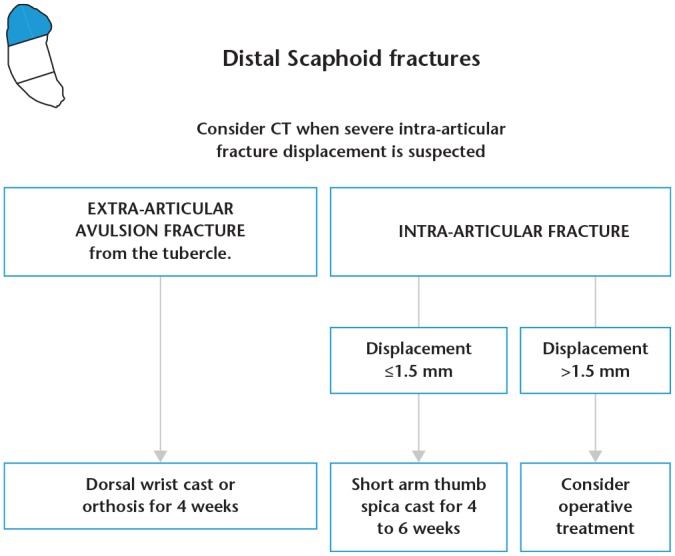
In cases of suspected scaphoid fracture where the initial radiographs are negative, a supplementary MRI, or alternatively CT, should be carried out within three to five days.Fracture classification, assessment of dislocation as well as evaluation of fracture healing is best done on CT with reconstructions in the coronal and sagittal planes, following the longitudinal axis of the scaphoid.After adequate conservative management, union is achieved at six weeks for approximately 90% of non-displaced or minimally displaced (≤ 0.5 mm) scaphoid waist fractures.Scaphoid waist fractures with moderate displacement (0.5-1.5 mm) can be treated conservatively, but require prolonged cast immobilization for approximately eight to ten weeks.Internal fixation is recommended for all scaphoid waist fractures with dislocation ≥ 1.5 mm.Distal scaphoid fractures can be treated conservatively. The majority heal uneventfully after four to six weeks of immobilization, depending on fracture type.In general, proximal scaphoid fractures should be treated with internal fixation. Cite this article: EFORT Open Rev 2020;5:96-103. DOI: 10.1302/2058-5241.5.190025.
Keywords: internal fixation; non-operative treatment; scaphoid fracture.
© 2020 The author(s).
Conflict of interest statement
ICMJE Conflict of interest statement: The authors declare no conflict of interest relevant to this work.
Figures
References
-
- Hove LM. Epidemiology of scaphoid fractures in Bergen, Norway. Scand J Plast Reconstr Surg Hand Surg 1999;33:423–426. - PubMed
-
- Jørgsholm P, Thomsen NO, Besjakov J, Abrahamsson SO, Björkman A. The benefit of magnetic resonance imaging for patients with posttraumatic radial wrist tenderness. J Hand Surg Am 2013;38:29–33. - PubMed
-
- Amirfeyz R, Bebbington A, Downing ND, Oni JA, Davis TR. Displaced scaphoid waist fractures: the use of a week 4 CT scan to predict the likelihood of union with nonoperative treatment. J Hand Surg Eur Vol 2011;36:498–502. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
