

Role of CT imaging in left atrial appendage occlusion for the WATCHMAN™ device
- PMID: 32175227
- PMCID: PMC7044092
- DOI: 10.21037/cdt.2019.12.01
Role of CT imaging in left atrial appendage occlusion for the WATCHMAN™ device
Abstract
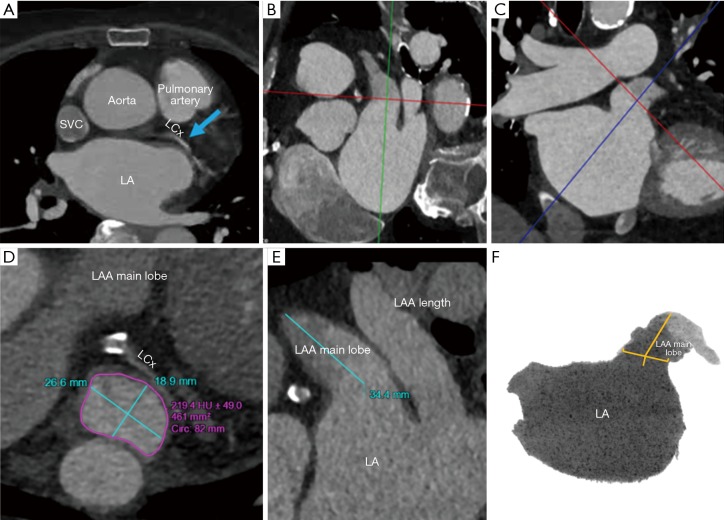
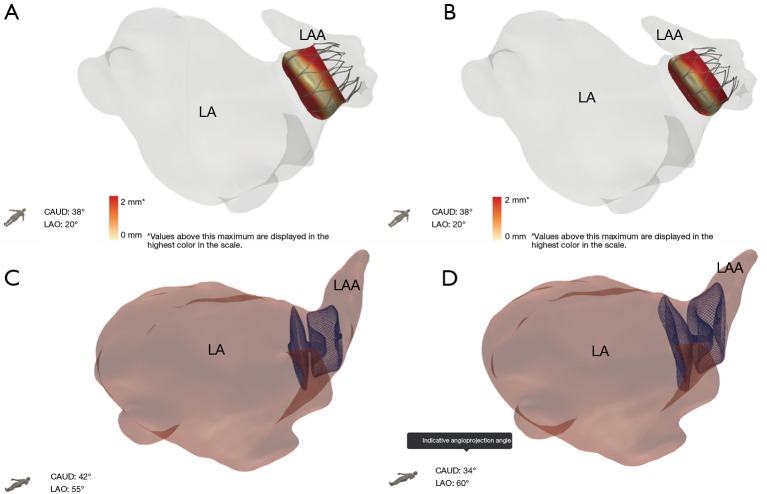
Computed tomography (CT) plays a key role in the peri-procedural planning of left atrial appendage occlusion (LAAO) device placement and post-procedural evaluation. The geometric variability of the interatrial septum, left atrium, and the left atrial appendage morphology can be fully visualized and intuitively appreciated through CT-derived, patient-specific 3D model unique to each individual's anatomy. This review further defines the strengths and limitations of CT peri-procedural imaging in the planning of LAAO.
Keywords: 3D modeling; 3D transesophageal echocardiogram; Left atrial appendage occlusion; WATCHMAN™ device; artifact; computerized tomography.
2020 Cardiovascular Diagnosis and Therapy. All rights reserved.
Conflict of interest statement
Conflicts of Interest: Dr. Wang is a consultant for Boston Scientific and receives research grant funding assigned to employer HFHS from Boston Scientific. Dr. O’Neill has served as a consultant for Edwards Lifesciences, Medtronic, Boston Scientific, Abbott Vascular and St. Jude Medical; and serves on the Board of Directors of Neovasc Inc. Dr Daniels is a consultant for WL Gore. Dr. Saw is a proctor, consultant and has received research grants from Boston Scientific and Abbott Vascular; and is on advisory boards for FEops, Baylis, Abiomed, Bayer, AstraZeneca, and Gore. Sanel Kesinovic and Tony Lamorgese are employees of Boston Scientific. All other authors report no relevant financial disclosures.
Figures
References
-
- Reiffel JA. Atrial fibrillation and stroke: epidemiology. Am J Med 2014;127:e15-6. - PubMed
-
- January CT, Wann S, Alpert JS, et al. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. Circulation 2014;130:2071-104. 10.1161/CIR.0000000000000040 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources