

Review of alternative access in transcatheter aortic valve replacement
- PMID: 32175229
- PMCID: PMC7044091
- DOI: 10.21037/cdt.2019.10.01
Review of alternative access in transcatheter aortic valve replacement
Abstract
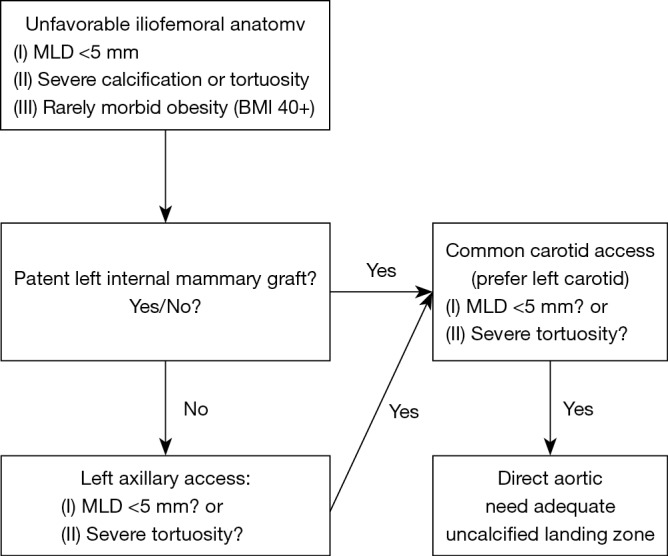
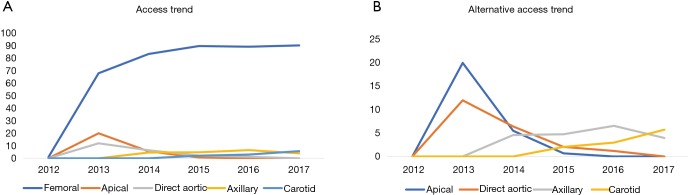
Transcatheter aortic valve replacement (TAVR) has surpassed surgical aortic valve replacement (SAVR) as the most common treatment strategy for severe symptomatic aortic stenosis over the past decade. As TAVR technology has continued to advance, it has been expanded from being an option only for extreme risk patients to now being the preferred option for the majority of patients with severe aortic stenosis. Recent trials have shown that TAVR is superior or non-inferior to SAVR even in patients at low surgical risk. One limitation of TAVR is the need for large bore vascular access. This has improved over time with smaller sheath sizes and improved delivery systems, but is still a significant issue in a patient population that often has many comorbidities including peripheral arterial disease. Early in the TAVR experience the only option for alternative access was transapical access, which has consistently been linked to increased procedural complications and worsened clinical outcomes. However, in recent years several centers have demonstrated the safety and efficacy of several alternative access strategies including transaxillary, transcarotid, transcaval, and direct aortic. There are no randomized data comparing these strategies, so access site approach is chosen by the multidisciplinary heart team based on patient anatomy and site expertise. We will review the current data in alternative access that in our view supports prioritizing a transaxillary or transcarotid strategy. In addition, we will describe our center's pre-procedural planning, peri-procedural approach, and propose an algorithm for alternative access.
Keywords: Transcatheter aortic valve replacement (TAVR); vascular access.
2020 Cardiovascular Diagnosis and Therapy. All rights reserved.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous