

Differentiation combined hepatocellular and cholangiocarcinoma from intrahepatic cholangiocarcinoma based on radiomics machine learning
- PMID: 32175412
- PMCID: PMC7049063
- DOI: 10.21037/atm.2020.01.126
Differentiation combined hepatocellular and cholangiocarcinoma from intrahepatic cholangiocarcinoma based on radiomics machine learning
Abstract
Background: Combined hepatocellular and cholangiocarcinoma (CHC) and intrahepatic cholangiocarcinoma (ICC) are hard to identify in clinical practice preoperatively. This study looked to develop and confirm a radiomics-based model for preoperative differentiation CHC from ICC.
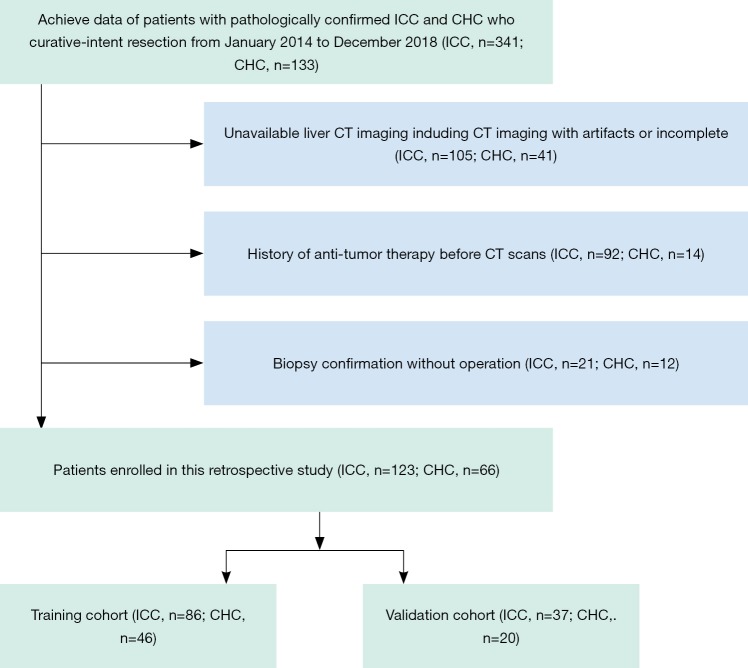
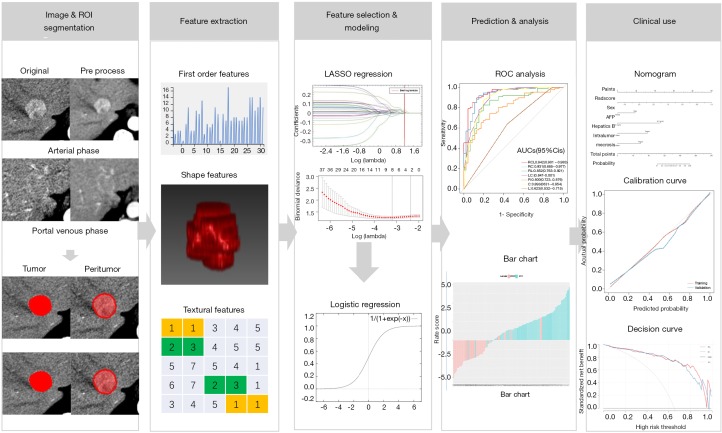
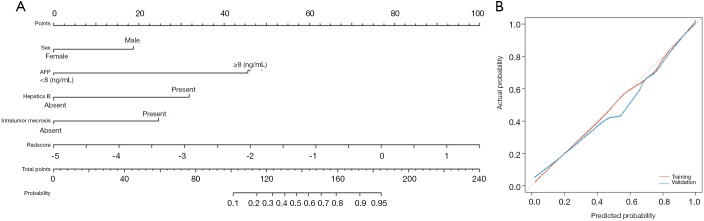
Methods: The model was developed in 86 patients with ICC and 46 CHC, confirmed in 37 ICC and 20 CHC, and data were collected from January 2014 to December 2018. The radiomics scores (Radscores) were built from radiomics features of contrast-enhanced computed tomography in 12 regions of interest (ROI). The Radscore and clinical-radiologic factors were integrated into the combined model using multivariable logistic regression. The best-combined model constructed the radiomics-based nomogram, and the performance was assessed concerning its calibration, discrimination, and clinical usefulness.
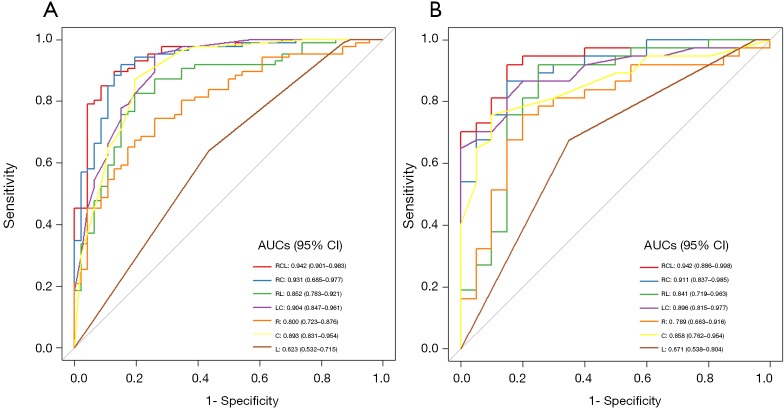
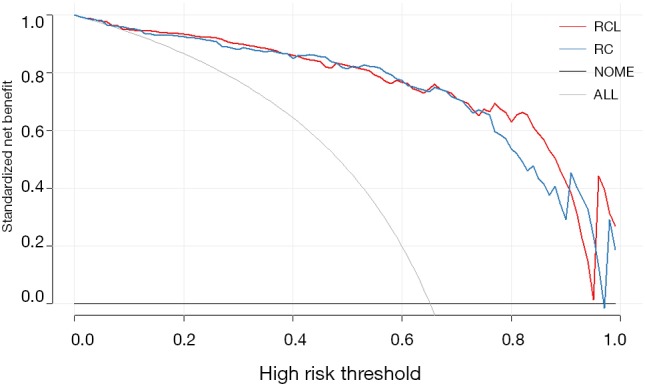
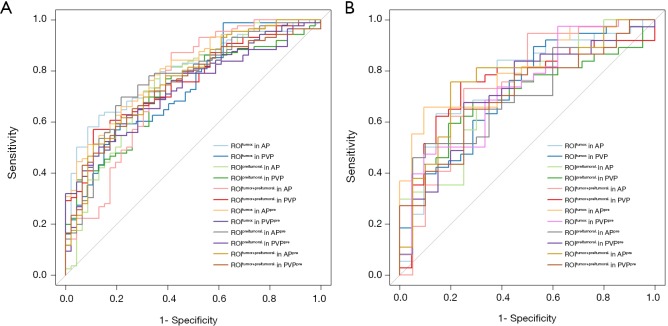
Results: The radiomics features extracted from tumor ROI in the arterial phase (AP) with preprocessing were selected to build Radscore and yielded an area under the curve (AUC) of 0.800 and 0.789 in training and validation cohorts, respectively. The radiomics-based model contained Radscore and 4 clinical-radiologic factors showed the best performance (training cohort, AUC =0.942; validation cohort, AUC =0.942) and good calibration (training cohort, AUC =0.935; validation cohort, AUC =0.931).
Conclusions: The proposed radiomics-based model may be used conveniently to the preoperatively differentiate CHC from ICC.
Keywords: Combined hepatocellular and cholangiocarcinoma (CHC); intrahepatic cholangiocarcinoma (ICC); machine learning; radiomics.
2020 Annals of Translational Medicine. All rights reserved.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
Similar articles
-
A radiomic-based model of different contrast-enhanced CT phase for differentiate intrahepatic cholangiocarcinoma from inflammatory mass with hepatolithiasis.Abdom Radiol (NY). 2021 Aug;46(8):3835-3844. doi: 10.1007/s00261-021-03027-6. Epub 2021 Mar 17. Abdom Radiol (NY). 2021. PMID: 33728532
-
DCE-MRI based radiomics nomogram for preoperatively differentiating combined hepatocellular-cholangiocarcinoma from mass-forming intrahepatic cholangiocarcinoma.Eur Radiol. 2022 Jul;32(7):5004-5015. doi: 10.1007/s00330-022-08548-2. Epub 2022 Feb 7. Eur Radiol. 2022. PMID: 35128572
-
Preoperative Computed Tomography Radiomics-Based Models for Predicting Microvascular Invasion of Intrahepatic Mass-Forming Cholangiocarcinoma.J Comput Assist Tomogr. 2025 May-Jun 01;49(3):358-366. doi: 10.1097/RCT.0000000000001686. Epub 2024 Nov 13. J Comput Assist Tomogr. 2025. PMID: 39761501
-
The Application Status of Radiomics-Based Machine Learning in Intrahepatic Cholangiocarcinoma: Systematic Review and Meta-Analysis.J Med Internet Res. 2025 May 5;27:e69906. doi: 10.2196/69906. J Med Internet Res. 2025. PMID: 40323647 Free PMC article. Review.
-
Radiomics predicting immunohistochemical markers in primary hepatic carcinoma: Current status and challenges.Heliyon. 2024 Nov 20;10(23):e40588. doi: 10.1016/j.heliyon.2024.e40588. eCollection 2024 Dec 15. Heliyon. 2024. PMID: 39660185 Free PMC article. Review.
Cited by
-
Morbidity, Prognostic Factors, and Competing Risk Nomogram for Combined Hepatocellular-Cholangiocarcinoma.J Oncol. 2021 Dec 10;2021:3002480. doi: 10.1155/2021/3002480. eCollection 2021. J Oncol. 2021. PMID: 34925507 Free PMC article.
-
The significance of the predominant component in combined hepatocellular-cholangiocarcinoma: MRI manifestation and prognostic value.Radiol Med. 2023 Sep;128(9):1047-1060. doi: 10.1007/s11547-023-01682-x. Epub 2023 Jul 20. Radiol Med. 2023. PMID: 37474663
-
Artificial intelligence and cholangiocarcinoma: Updates and prospects.World J Clin Oncol. 2022 Feb 24;13(2):125-134. doi: 10.5306/wjco.v13.i2.125. World J Clin Oncol. 2022. PMID: 35316928 Free PMC article. Review.
-
The clinical characteristics and prognostic factors of combined Hepatocellular Carcinoma and Cholangiocarcinoma, Hepatocellular Carcinoma and Intrahepatic Cholangiocarcinoma after Surgical Resection: A propensity score matching analysis.Int J Med Sci. 2021 Jan 1;18(1):187-198. doi: 10.7150/ijms.50883. eCollection 2021. Int J Med Sci. 2021. PMID: 33390787 Free PMC article.
-
Radiomics of Biliary Tumors: A Systematic Review of Current Evidence.Diagnostics (Basel). 2022 Mar 28;12(4):826. doi: 10.3390/diagnostics12040826. Diagnostics (Basel). 2022. PMID: 35453878 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources