

State Variability in the Prevalence and Healthcare Utilization of Assisted Living Residents with Dementia
- PMID: 32175594
- PMCID: PMC7363564
- DOI: 10.1111/jgs.16410
State Variability in the Prevalence and Healthcare Utilization of Assisted Living Residents with Dementia
Abstract
Objectives: Almost 1 million older and disabled adults who require long-term care reside in assisted living (AL), approximately 40% of whom have a diagnosis of Alzheimer's disease and related dementias (ADRD). States vary in their regulations specific to dementia care that may influence the presence of residents with ADRD in AL and their outcomes. The objectives of this study were to describe the state variability in the prevalence of ADRD among Medicare beneficiaries residing in larger (25+ bed) ALs and their healthcare utilization.
Design: Retrospective observational national study.
Participants: National cohort of 293,336 Medicare fee-for-service enrollees residing in larger (25+ bed) ALs in 2016 and 2017 including 88,867 (30.3%) residents with ADRD. We compared this cohort's characteristics and healthcare utilization with that of individuals with ADRD who resided in nursing homes (NHs; n = 602,521) and the community (n = 2,074,420).
Methods: Medicare enrollment data, claims, and the NH Minimum Data Set were used to describe differences among ADRD patients in AL, NHs, and the community. We present rates of NH admission and hospitalization, by state, adjusting for age, sex, race, dual eligibility, and chronic conditions.
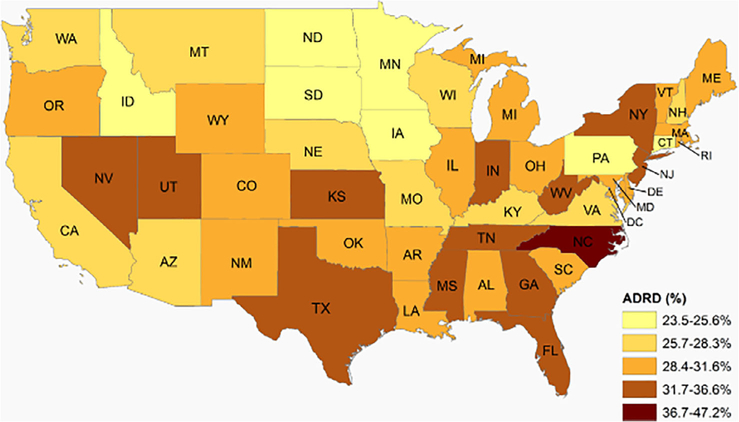
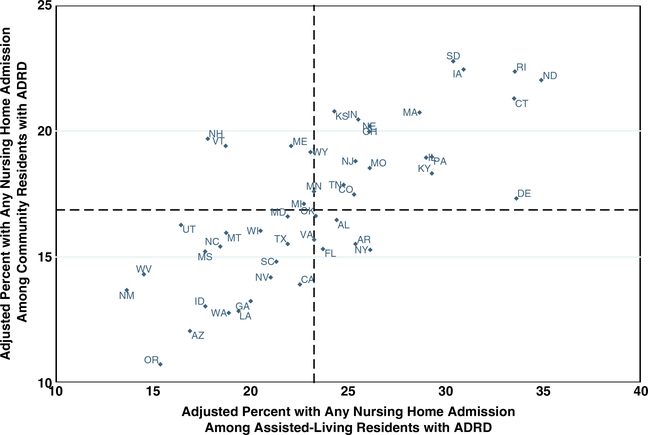
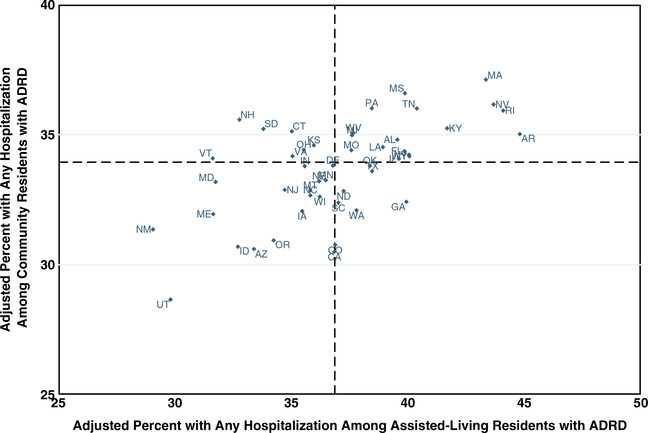
Results: The prevalence of ADRD among AL residents varied by state, ranging from 24% to 47%. In 2017, AL residents with ADRD had higher rates of NH admission than their community-dwelling counterparts (adjusted national average = 24%, ranging from 14% to 35% among states). AL residents with ADRD had higher rates of hospitalization (38%) than populations in either NHs (29%) or the community (34%), and ranged from 29% to 45% of residents among states.
Conclusion: These findings have implications for states as they regulate AL and for healthcare professionals whose patients reside in AL. Future work is needed to understand specific elements of states' regulatory environments and local markets that may impact access and outcomes for this vulnerable population of residents with ADRD. J Am Geriatr Soc 68:1504-1511, 2020.
Keywords: Alzheimer's disease and related dementias; assisted living; long-term care.
© 2020 The American Geriatrics Society.
Conflict of interest statement
Figures
References
-
- Harris-Kojetin L,Sengupta M,Lendon JP, Rome V,Valverde R, Caffrey C.Long-term care providers and services users in the United States, 2015–2016. National Center for Health Statistics. Vital Health Stat. 2019;3(43). https://www.cdc.gov/nchs/data/series/sr_03/sr03_43-508.pdf. Accessed October 9, 2019. - PubMed
-
- Zimmerman S, Sloane PD, Reed D. Dementia prevalence and care in assistedliving. Health Aff (Millwood). 2014. 33(4):658–666. - PubMed
-
- Magsi H, Malloy T. Under-recognition of cognitive impairment in assistedliving facilities. J Am Geriatr Soc. 2005;53(2):295–298. - PubMed
-
- Caffrey C, Sengupta M, Park-Lee E, Moss A, Rosenhoff E, Harris-Kojetin L.Residents living in residential care facilities: United States, 2010. NCHS Data Brief. 2012;(91):1–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
