

Inpatient Respiratory Arrest Associated With Sedative and Analgesic Medications: Impact of Continuous Monitoring on Patient Mortality and Severe Morbidity
- PMID: 32175965
- PMCID: PMC8612899
- DOI: 10.1097/PTS.0000000000000696
Inpatient Respiratory Arrest Associated With Sedative and Analgesic Medications: Impact of Continuous Monitoring on Patient Mortality and Severe Morbidity
Abstract
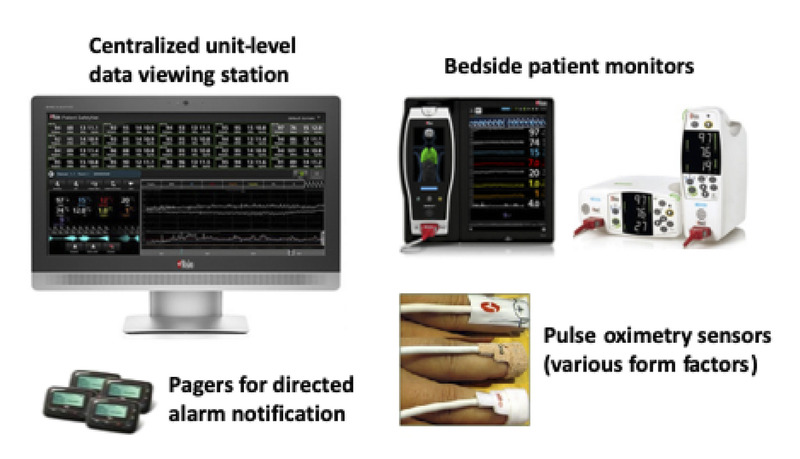
Objectives: The primary study objective was to investigate the impact of surveillance monitoring (i.e., continuous monitoring optimized for deterioration detection) on mortality and severe morbidity associated with administration of sedative/analgesic medications in the general care setting. A second objective was consideration of the results in the context of previous investigations to establish practice recommendations for this approach to patient safety.
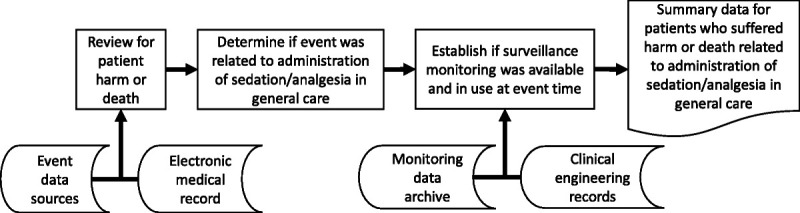
Methods: Retrospective review of available rescue event and patient safety data from a tertiary care hospital in a rural setting was performed for a 10-year period. Systematic analysis of all adult general care inpatient data followed by chart review for individual patients was used to identify patient death or permanent harm (i.e., ventilator dependency, hypoxic encephalopathy) related to administration of sedative/analgesics.
Results: Of 111,488 patients in units with surveillance monitoring available, none died or were harmed by opioid-induced respiratory depression when surveillance monitoring was in use. One patient died from opioid-induced respiratory depression in a unit where surveillance monitoring was available; however, the patient was not monitored at the time of the adverse event. In unmonitored units (15,209 patients during 29 months of incremental implementation), three patients died from opioid overdose (19.73 deaths per 100,000 at risk patients). The reduced death rate when surveillance monitoring was available (0.0009%) versus not available (0.02%) was significant (P = 0.03).
Conclusions: For a 10-year period, the rescue system with continuous surveillance monitoring had a profound effect on death from sedative/analgesic administration in the general care setting. This approach to patient safety can help address the risk of sedative/analgesic-related respiratory arrests in hospitals.
Copyright © 2020 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The other authors disclose no potential conflict of interest.
Figures
References
-
- Macintyre PE, Loadsman JA, Scott DA. Opioids, ventilation and acute pain management. Anaesth Intensive Care. 2011;39:545–558. - PubMed
-
- Freeman WJ, Weiss AJ, Heslin KC. Overview of U.S. Hospital Stays in 2016: Variation by Geographic Region. HCUP Statistical Brief #246. [Internet]. Rockville, MD: Agency for Healthcare Research and Quality; 2018. Available at: https://www.hcup-us.ahrq.gov/reports/statbriefs/sb246-Geographic-Variati.... Accessed February 28, 2020. - PubMed
-
- Pasero C. Opioid-induced sedation and respiratory depression: evidence-based monitoring guidelines. J Perianesth Nurs. 2012;27:208–211. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
