

What is the relevance of an ambulatory quick diagnosis unit or inpatient admission for the diagnosis of pancreatic cancer? A retrospective study of 1004 patients
- PMID: 32176029
- PMCID: PMC7440208
- DOI: 10.1097/MD.0000000000019009
What is the relevance of an ambulatory quick diagnosis unit or inpatient admission for the diagnosis of pancreatic cancer? A retrospective study of 1004 patients
Abstract
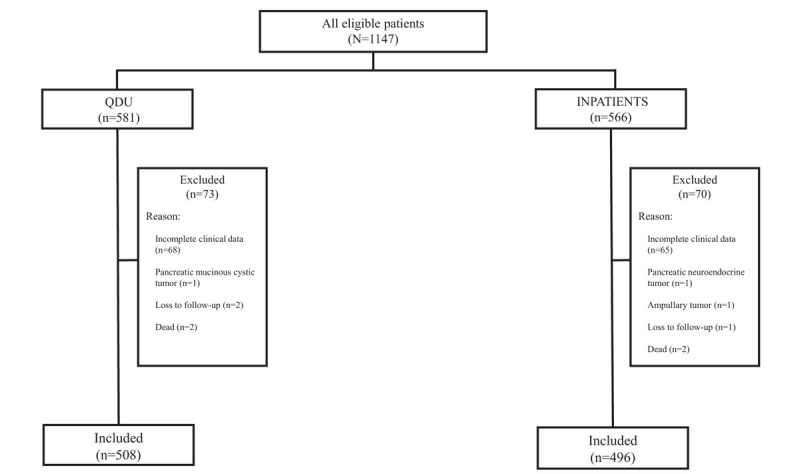
Quick diagnosis units (QDU) have become an alternative hospital-based ambulatory medicine strategy to inpatient hospitalization for potentially serious illnesses in Spain. Whether diagnosis of pancreatic cancer is better accomplished by an ambulatory or inpatient approach is unknown. The main objective of this retrospective study was to examine and compare the diagnostic effectiveness of a QDU or inpatient setting in patients with pancreatic cancer.Patients with a diagnosis of pancreatic adenocarcinoma who had been referred to a university, tertiary hospital-based QDU or hospitalized between 2005 and 2018 were eligible. Presenting symptoms and signs, risk and prognostic factors, and time to diagnosis were compared. The costs incurred during the diagnostic assessment were analyzed with a microcosting method.A total of 1004 patients (508 QDU patients and 496 inpatients) were eligible. Admitted patients were more likely than QDU patients to have weight loss, asthenia, anorexia, abdominal pain, jaundice, and palpable hepatomegaly. Time to diagnosis of inpatients was similar to that of QDU patients (4.1 [0.8 vs 4.3 [0.6] days; P = .163). Inpatients were more likely than QDU patients to have a tumor on the head of the pancreas, a tumor size >2 cm, a more advanced nodal stage, and a poorer histological differentiation. No differences were observed in the proportion of metastatic and locally advanced disease and surgical resections. Microcosting revealed a cost of &OV0556;347.76 (48.69) per QDU patient and &OV0556;634.36 (80.56) per inpatient (P < .001).Diagnosis of pancreatic cancer is similarly achieved by an inpatient or QDU clinical approach, but the latter seems to be cost-effective. Because the high costs of hospitalization, an ambulatory diagnostic assessment may be preferable in these patients.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Kamisawa T, Wood LD, Itoi T, et al. Pancreatic cancer. Lancet 2016;388:73–85. - PubMed
-
- Ducreux M, Cuhna AS, Caramella C, et al. ESMO Guidelines Committee. Cancer of the pancreas: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol 2015;26: Suppl 5: v56–68. - PubMed
-
- Ryan DP, Hong TS, Bardeesy N. Pancreatic adenocarcinoma. N Engl J Med 2014;371:1039–49. - PubMed
-
- Maroni L, Ravaioli M, Pinna AD. Why is pancreatic adenocarcinoma not screened for earlier? Expert Rev Anticancer Ther 2016;16:1003–4. - PubMed
