

Male axillary accessory breast cancer: A case report
- PMID: 32176095
- PMCID: PMC7440245
- DOI: 10.1097/MD.0000000000019506
Male axillary accessory breast cancer: A case report
Abstract
Rationale: Accessory breast cancer is extremely rare among all cancerous diseases, especially in male patients. There were only few male axillary accessory breast cancer cases that have been reported in scientific literatures so far. Hereby, we would like to discuss a case of male axillary accessory breast cancer found in our hospital.
Patient concerns: We report a male senile patient suffering from a painful, enlarged, and hardened right axillary mass for more than 20 years. He came for further treatments due to progressive growth of the mass for 11 months with bloody ulceration for more than 1 month.
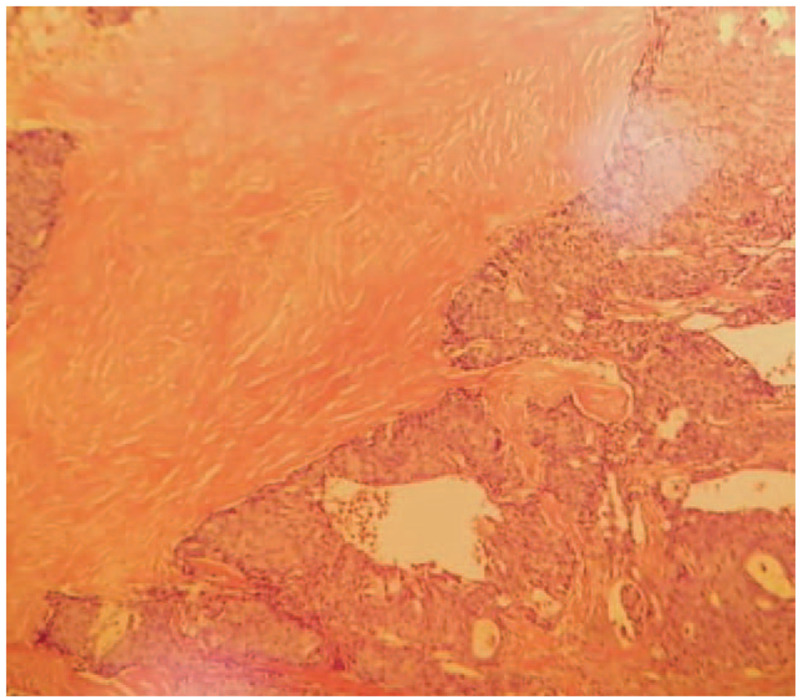
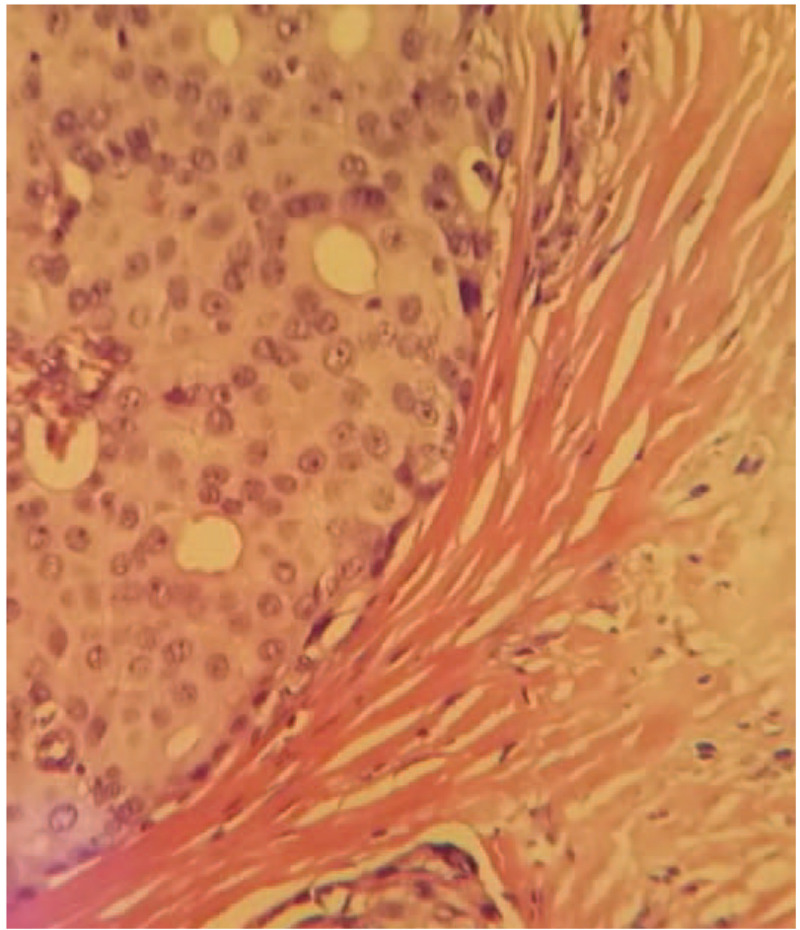
Diagnosis: Pathological examination manifested a grade II infiltrating ductal carcinoma derived from the accessory mammary gland (right axilla), with invasion of local skin. Immunohistochemical examination result: estrogen receptor (++) 90%, progesterone receptor (+++) 100%, human epidermal growth factor receptor-2 (1+), ki67 (20% positive), prostate specific antigen (-), caudal-related homeobox-2 (-), thyroid transcription factor-1 (-), Synaptophysin (+), NapsinA (1), and CK7 (-).
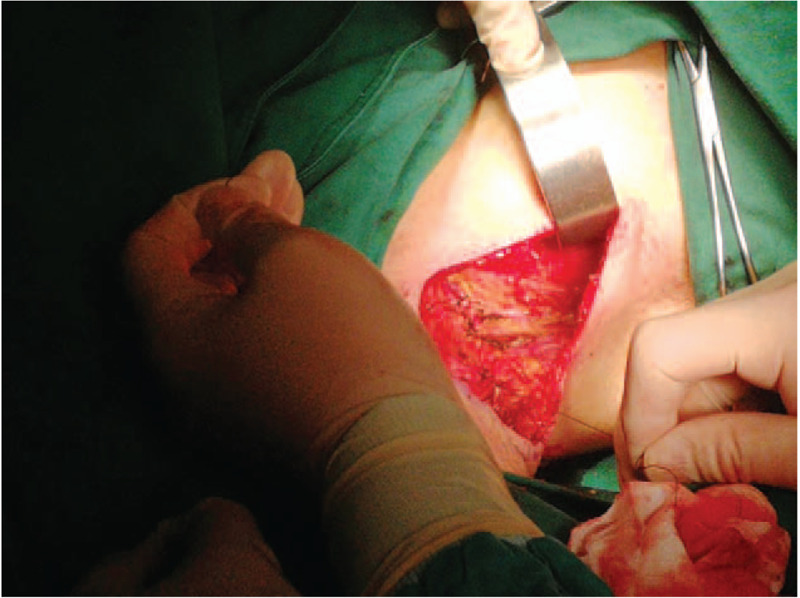
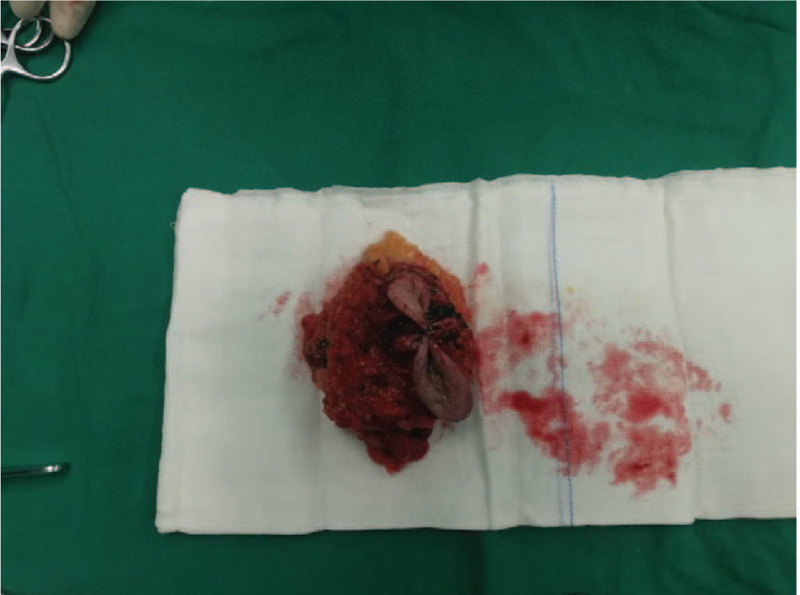
Interventions: Modified radical mastectomy and axillary lymph nodes clearance were performed on the accessary breast cancer under general anesthesia. Postoperatively, endocrine therapy was provided for the patient, orally-taken Letrozole was recommended for the rest of the patient's life.
Outcomes: The patient recovered uneventfully and was discharged 3 days after the operation. The patient continued to take Letrozole orally regularly at home and no signs of recurrence were observed.
Conclusion: Axillary accessory breast cancer in males is extremely rare, with no conspicuous and typical clinical presentations, which leads to inevitable neglect by clinicians. Therefore, there is significant necessity for clinicians to be cautious with this type of disease.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures

Similar articles
-
Optimal sentinel node examination and a new strategy for axillary control in breast cancer.Breast J. 2002 Jan-Feb;8(1):10-4. doi: 10.1046/j.1524-4741.2002.08003.x. Breast J. 2002. PMID: 11856155
-
Male occult breast cancer with axillary lymph node metastasis as the first manifestation: A case report and literature review.Medicine (Baltimore). 2017 Dec;96(51):e9312. doi: 10.1097/MD.0000000000009312. Medicine (Baltimore). 2017. PMID: 29390502 Free PMC article. Review.
-
Male occult triple-negative breast cancer.BMJ Case Rep. 2019 Apr 20;12(4):e229482. doi: 10.1136/bcr-2019-229482. BMJ Case Rep. 2019. PMID: 31005873 Free PMC article.
-
CDX2-positive breast cancer presented with axillary lymph node metastases: A case report.Cancer Treat Res Commun. 2021;26:100300. doi: 10.1016/j.ctarc.2020.100300. Epub 2020 Dec 29. Cancer Treat Res Commun. 2021. PMID: 33421821
-
Occult breast cancer presenting axillary nodal metastasis: a case report.Jpn J Clin Oncol. 2000 Apr;30(4):185-7. doi: 10.1093/jjco/hyd047. Jpn J Clin Oncol. 2000. PMID: 10830987 Review.
Cited by
-
Diagnosis and Treatment of Male Accessory Breast Cancer: A Comprehensive Systematic Review.Front Oncol. 2021 Mar 29;11:640000. doi: 10.3389/fonc.2021.640000. eCollection 2021. Front Oncol. 2021. PMID: 33854973 Free PMC article.
-
Male triple negative axillary accessory breast cancer-a case report.Transl Cancer Res. 2022 Aug;11(8):2926-2930. doi: 10.21037/tcr-22-33. Transl Cancer Res. 2022. PMID: 36093543 Free PMC article.
-
Ectopic Male Breast Cancer in Suprapubic Area That Relapsed with Hematogenous Metastasis.J Breast Cancer. 2021 Jun;24(3):344-348. doi: 10.4048/jbc.2021.24.e21. Epub 2021 Apr 12. J Breast Cancer. 2021. PMID: 34128361 Free PMC article.
-
Axillary masses as clinical manifestations of male sweat gland carcinoma associated with extramammary Paget's disease and accessory breast carcinoma: two cases report and literature review.World J Surg Oncol. 2022 Apr 4;20(1):109. doi: 10.1186/s12957-022-02570-w. World J Surg Oncol. 2022. PMID: 35379255 Free PMC article. Review.
-
Axillary Reverse Lymphatic Mapping in the Treatment of Axillary Accessory Breast Cancer: A Case Report and Review of Management.Eur J Breast Health. 2021 Dec 30;18(1):1-5. doi: 10.4274/ejbh.galenos.2021.2021-7-3. eCollection 2022 Jan. Eur J Breast Health. 2021. PMID: 35059584 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
