

Association of a Lay Health Worker Intervention With Symptom Burden, Survival, Health Care Use, and Total Costs Among Medicare Enrollees With Cancer
- PMID: 32176306
- PMCID: PMC7076340
- DOI: 10.1001/jamanetworkopen.2020.1023
Association of a Lay Health Worker Intervention With Symptom Burden, Survival, Health Care Use, and Total Costs Among Medicare Enrollees With Cancer
Abstract
Importance: Undertreated patient symptoms require approaches that improve symptom burden.
Objective: To determine the association of a lay health worker-led symptom screening and referral intervention with symptom burden, survival, health care use, and total costs among Medicare Advantage enrollees with a new diagnosis of solid or hematologic malignant neoplasms.
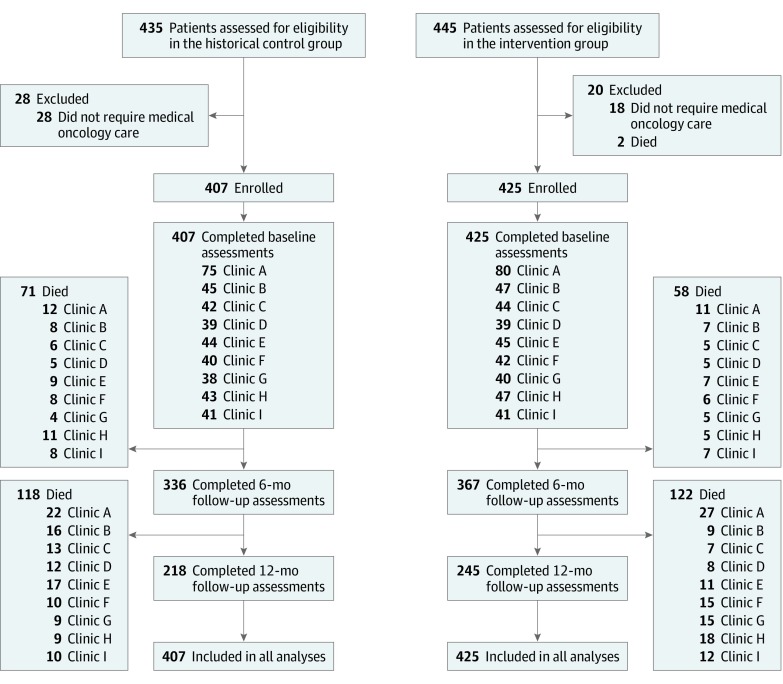
Design, setting, and participants: This quality improvement study conducted at 9 community oncology practices from November 1, 2016, to October 31, 2018, compared newly diagnosed Medicare Advantage enrollees with solid or hematologic malignant neoplasms with patients diagnosed and treated 1 year prior. Analysis was conducted from August 1, 2019, to January 11, 2020.
Interventions: Usual care augmented by a lay health worker trained to screen symptoms and refer patients to palliative care and behavioral medicine.
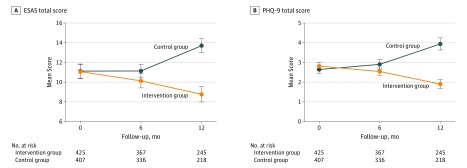
Main outcomes and measures: The primary outcome was change in symptoms using the Edmonton Symptom Assessment Scale and the 9-item Patient Health Questionnaire at baseline and 6 and 12 months after enrollment. Secondary outcomes were between-group comparison of survival, 12-month health care use, and costs.
Results: Among 425 patients in the intervention group and 407 patients in the control group, the mean (SD) age was 78.8 (8.3) years, 345 (41.5%) were female, and 407 (48.9%) were non-Hispanic white. Patients in the intervention group experienced a lower symptom burden as measured by the Edmonton Symptom Assessment Scale score over time compared with patients in the control group (mean [SD] difference, -1.9 [14.2]; 95% CI, -3.77 to -0.19; P = .01 for the intervention group and 2.32 [17.7]; 95% CI, 0.47 to 4.19; P = .02 for the control group). Similar findings were noted in 9-item Patient Health Questionnaire depression scores (mean [SD] difference, -0.63 [3.99]; 95% CI, -1.23 to -0.028; P = .04 for the intervention group and 1.67 [5.49]; 95% CI, 0.95 to 2.37; P = .01 for the control group). Patients in the intervention group compared with patients in the control group had fewer mean (SD) inpatient visits (0.54 [0.77]; 95% CI, 0.47-0.61 vs 0.72 [1.12]; 95% CI, 0.61-0.83; P = .04) and emergency department visits (0.43 [0.76]; 95% CI, 0.36-0.50 vs 0.57 [1.00]; 95% CI, 0.48-0.67; P = .002) per 1000 patients per year and lower total costs (median, $17 869 [interquartile range, $6865-$32 540] vs median, $18 473 [interquartile range, $6415-$37 910]; P = .02). A total of 180 patients in the intervention group and 189 patients in the control group died within 12 months. Among those who died, patients in the intervention group had greater hospice use (125 of 180 [69.4%] vs 79 of 189 [41.8%]; odds ratio, 3.16; 95% CI, 2.13-4.69; P < .001), fewer mean (SD) emergency department and hospital visits (emergency department: 0.10 [0.30]; 95% CI, 0.06-0.14 vs 0.30 [0.46]; 95% CI, 0.24-0.38; P = .001; hospital: 0.27 [0.44]; 95% CI, 0.21-0.34 vs 0.43 [0.82]; 95% CI, 0.32-0.55; P = .02), and lower costs (median, $3602 [interquartile range, $1076-$9436] vs median, $12 726 [interquartile range, $5259-$22 170]; P = .002), but there was no significant difference in inpatient deaths (18 of 180 [10.0%] vs 30 of 189 [15.9%]; P = .14).
Conclusions and relevance: This study suggests that a lay health worker-led intervention may be one way to improve burdensome and costly care.
Conflict of interest statement
Figures
Similar articles
-
Lay Health Worker-Led Cancer Symptom Screening Intervention and the Effect on Patient-Reported Satisfaction, Health Status, Health Care Use, and Total Costs: Results From a Tri-Part Collaboration.JCO Oncol Pract. 2020 Jan;16(1):e19-e28. doi: 10.1200/JOP.19.00152. Epub 2019 Sep 24. JCO Oncol Pract. 2020. PMID: 31550213 Free PMC article.
-
Effect of an Oncology Nurse-Led Primary Palliative Care Intervention on Patients With Advanced Cancer: The CONNECT Cluster Randomized Clinical Trial.JAMA Intern Med. 2021 Nov 1;181(11):1451-1460. doi: 10.1001/jamainternmed.2021.5185. JAMA Intern Med. 2021. PMID: 34515737 Free PMC article. Clinical Trial.
-
Effect of a Lay Health Worker Intervention on Goals-of-Care Documentation and on Health Care Use, Costs, and Satisfaction Among Patients With Cancer: A Randomized Clinical Trial.JAMA Oncol. 2018 Oct 1;4(10):1359-1366. doi: 10.1001/jamaoncol.2018.2446. JAMA Oncol. 2018. PMID: 30054634 Free PMC article. Clinical Trial.
-
Association of Receipt of Palliative Care Interventions With Health Care Use, Quality of Life, and Symptom Burden Among Adults With Chronic Noncancer Illness: A Systematic Review and Meta-analysis.JAMA. 2020 Oct 13;324(14):1439-1450. doi: 10.1001/jama.2020.14205. JAMA. 2020. PMID: 33048152 Free PMC article.
-
Palliative care in advanced cancer patients: how and when?Oncologist. 2012;17(2):267-73. doi: 10.1634/theoncologist.2011-0219. Epub 2012 Jan 17. Oncologist. 2012. PMID: 22252934 Free PMC article. Review.
Cited by
-
Health Care Professionals' Perspectives on Implementation, Adoption, and Maintenance of a Community Health Worker-Led Advance Care Planning and Cancer Symptom Screening Intervention: A Qualitative Study.JCO Oncol Pract. 2023 Jan;19(1):e138-e149. doi: 10.1200/OP.22.00209. Epub 2022 Oct 6. JCO Oncol Pract. 2023. PMID: 36201710 Free PMC article.
-
Community health workers and precision medicine: A randomized controlled trial.Contemp Clin Trials. 2022 Oct;121:106906. doi: 10.1016/j.cct.2022.106906. Epub 2022 Sep 6. Contemp Clin Trials. 2022. PMID: 36084898 Free PMC article. Clinical Trial.
-
The Effects of Patient-Reported Outcome Screening on the Survival of People with Cancer: A Systematic Review and Meta-Analysis.Cancers (Basel). 2022 Nov 7;14(21):5470. doi: 10.3390/cancers14215470. Cancers (Basel). 2022. PMID: 36358888 Free PMC article. Review.
-
Lay Health Workers' Perspectives on Delivery of Advance Care Planning and Symptom Screening Among Adults With Cancer: A Qualitative Study.Am J Hosp Palliat Care. 2021 Oct;38(10):1202-1211. doi: 10.1177/1049909120977841. Epub 2020 Dec 3. Am J Hosp Palliat Care. 2021. PMID: 33267632 Free PMC article.
-
Healthcare delivery interventions to reduce cancer disparities worldwide.World J Clin Oncol. 2020 Sep 24;11(9):705-722. doi: 10.5306/wjco.v11.i9.705. World J Clin Oncol. 2020. PMID: 33033693 Free PMC article. Review.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
