

Validation of the 34-week gestation as definition of late onset preeclampsia: Testing different cutoffs from 30 to 37 weeks on a population-based cohort of 1700 preeclamptics
- PMID: 32176317
- PMCID: PMC7492422
- DOI: 10.1111/aogs.13846
Validation of the 34-week gestation as definition of late onset preeclampsia: Testing different cutoffs from 30 to 37 weeks on a population-based cohort of 1700 preeclamptics
Abstract
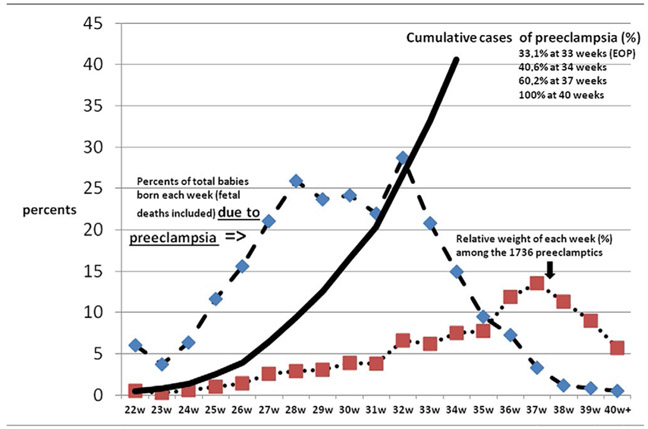
Introduction: Early onset preeclampsia (EOP) and late onset preeclampsia (LOP) have been differentiated with a cut-point of ≤34 weeks. This classical definition has never been examined with respect to maternal characteristics by different gestational age cut-points. We examined maternal characteristics in a population-based cohort of 1736 preeclamptic deliveries at different gestational age cut-points from 30 to 37 weeks (CO30 to CO37).
Material and methods: Eighteen-year observational population-based historical cohort study (2001-2018). All consecutive births delivered at the Centre Hospitalier Universitaire Hospitalier Sud Reunion's maternity. Standardized epidemiological perinatal database.
Results: The incidence of EOP was lower in adolescents (1.8% vs 3.5%, odds ratio [OR] 0.50, P = .17). Conversely, the odds of LOP was increased for women over 35, beginning at C030 (OR 1.13, P = .02) and this effect (OR = 1.2) was still detectable at C037 (P = .06). Among primigravid women, the incidence of EOP was lower than LOP (OR ranging from 0.71 to 0.82 for different CO). Conversely, the incidence of LOP was higher (adjusted OR about 2.7 [CO30-CO34] with a rise to 3.3 at CO37 (P < .001). Women with EOP had a lower body mass index (BMI) as compared with LOP at CO34 and CO37. The adjusted OR (per 5 kg/m2 increment) declined from 1.06 to 1.03 from CO30 to C037 in EOP women. Conversely, for LOP, the adjusted odds ratio (aOR) increased from 1.04 to 1.06 from CO30 to CO37 (P < .001). Gestational diabetes mellitus was not associated with LOP at any cut-off (aOR 1.07, NS) but was protective against EOP from CO30 to CO34 (aOR 0.42, 0.61 and 0.73, respectively, P < .001). This protective effect disappeared at CO37. Chronic hypertension and history of preeclampsia were both EOP and LOP risks but with a much stronger effect for EOP (chronic hypertension: aOR 6.0-6.5, history of preeclampsia: aOR 12-17).
Conclusions: The 34th week of gestation appears to provide a reasonable cut-point to differentiate between EOP and LOP. Additional research is needed to better describe the possible differences in the pathophysiology of these different phenotypes.
Keywords: early onset preeclampsia; epidemiology; late onset preeclampsia; preeclampsia.
© 2020 Nordic Federation of Societies of Obstetrics and Gynecology (NFOG). Published by John Wiley & Sons Ltd.
Conflict of interest statement
CONFLICT OF INTEREST
None.
Figures

References
-
- Ness RB, Roberts JM. Heterogeneous causes constituting the single syndrome of preeclampsia: a hypothesis and its implications. Am J Obstet Gynecol. 1996;175:1365–1370. - PubMed
-
- Burton GJ, Redman CW, Roberts JM, Moffett A. Pre-eclampsia: pathophysiology and clinical implications. BMJ. 2019;366:l2381. - PubMed
-
- Tranquilli AL, Brown MA, Zeeman GG, Dekker G, Sibai BM. The definition of severe and early-onset preeclampsia. Statements from the International Society for the Study of Hypertension in Pregnancy (ISSHP). Pregnancy Hypertens. 2013;3:44–47. - PubMed
-
- Robillard PY, Dekker G, Iacobelli S, Chaouat G. An essay of reflection: why does preeclampsia exist in humans, and why are there such huge geographical differences in epidemiology? J Reprod Immunol. 2016;114:44–47. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
