

Sepsis therapies: learning from 30 years of failure of translational research to propose new leads
- PMID: 32176432
- PMCID: PMC7136965
- DOI: 10.15252/emmm.201810128
Sepsis therapies: learning from 30 years of failure of translational research to propose new leads
Abstract
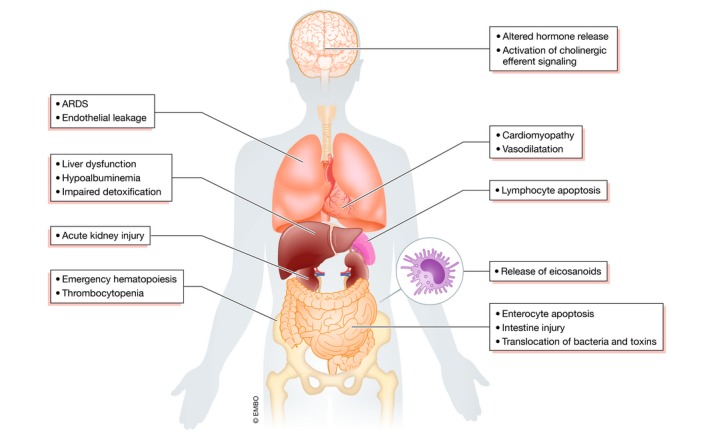
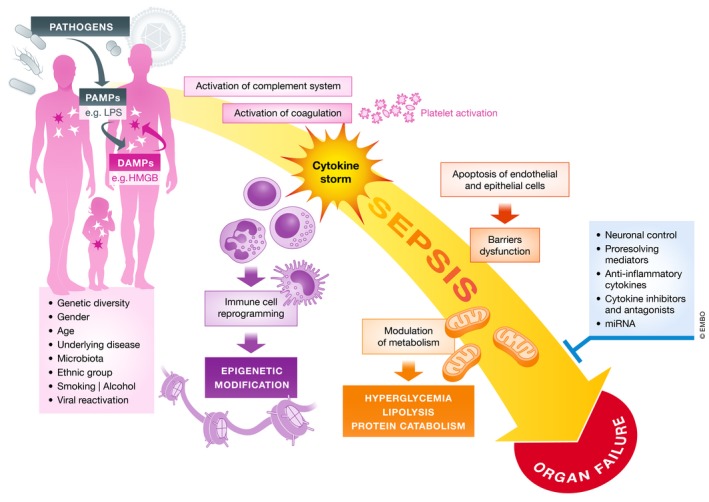
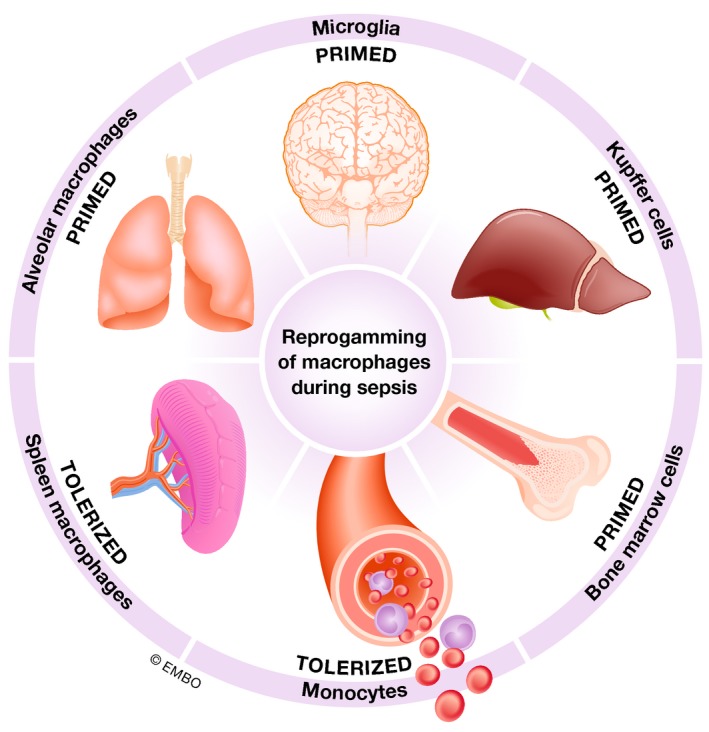
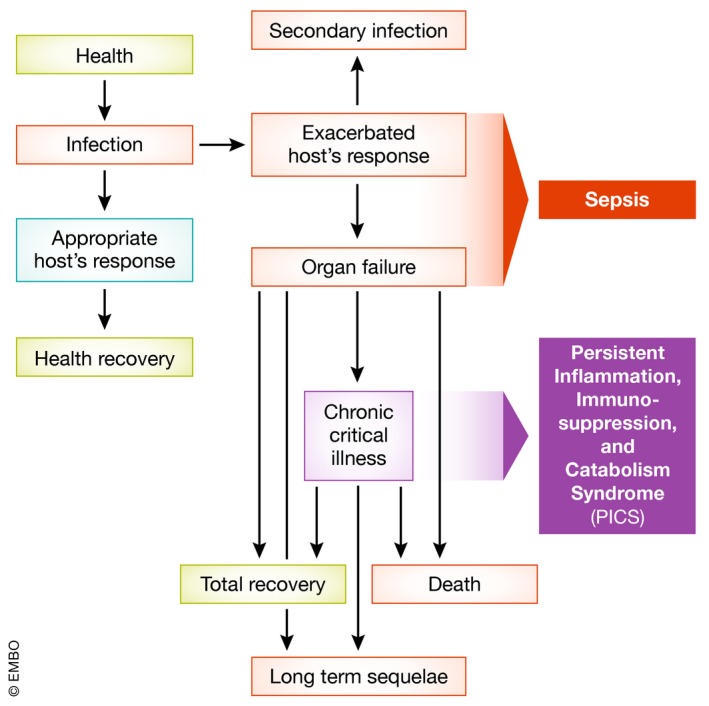
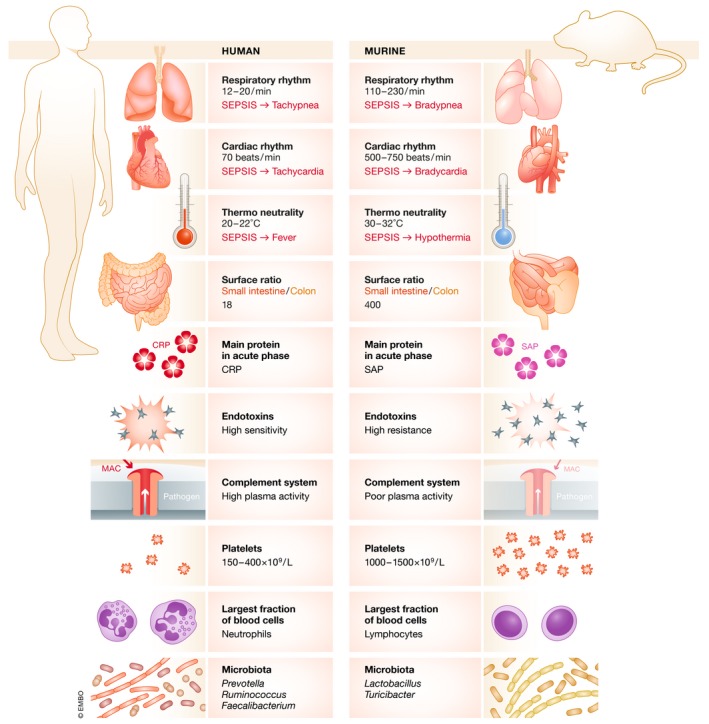
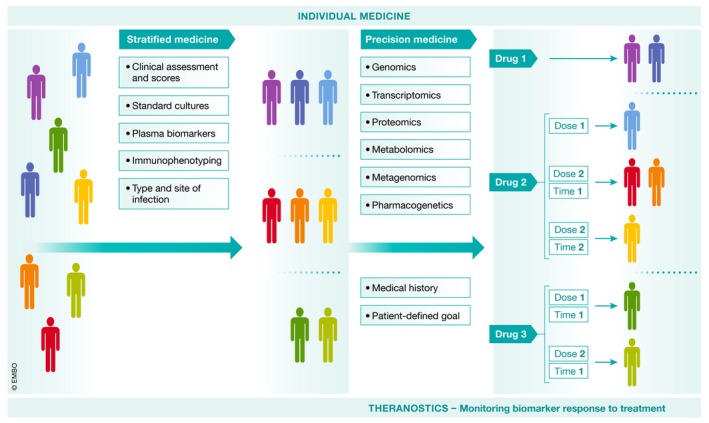
Sepsis has been identified by the World Health Organization (WHO) as a global health priority. There has been a tremendous effort to decipher underlying mechanisms responsible for organ failure and death, and to develop new treatments. Despite saving thousands of animals over the last three decades in multiple preclinical studies, no new effective drug has emerged that has clearly improved patient outcomes. In the present review, we analyze the reasons for this failure, focusing on the inclusion of inappropriate patients and the use of irrelevant animal models. We advocate against repeating the same mistakes and propose changes to the research paradigm. We discuss the long-term consequences of surviving sepsis and, finally, list some putative approaches-both old and new-that could help save lives and improve survivorship.
Keywords: animal models; cytokine storm; personalized medicine; reprogramming; sepsis.
© 2020 The Authors. Published under the terms of the CC BY 4.0 license.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Acker CG, Singh AR, Flick RP, Bernardini J, Greenberg A, Johnson JP (2000) A trial of thyroxine in acute renal failure. Kidney Int 57: 293–298 - PubMed
-
- Adembri C, Selmi V, Vitali L, Tani A, Margheri M, Loriga B, Carlucci M, Nosi D, Formigli L, De Gaudio AR (2014) Minocycline but not tigecycline is neuroprotective and reduces the neuroinflammatory response induced by the superimposition of sepsis upon traumatic brain injury. Crit Care Med 42: e570–e582 - PubMed
-
- Adib‐Conquy M, Adrie C, Fitting C, Gattoliat O, Beyaert R, Cavaillon JM (2006) Up‐regulation of MyD88s and SIGIRR, molecules inhibiting Toll‐like receptor signaling, in monocytes from septic patients. Crit Care Med 34: 2377–2385 - PubMed
-
- Andreis DT, Singer M (2016) Catecholamines for inflammatory shock: a Jekyll‐and‐Hyde conundrum. Intensive Care Med 42: 1387–1397 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
