

Blood transcriptional biomarkers for active pulmonary tuberculosis in a high-burden setting: a prospective, observational, diagnostic accuracy study
- PMID: 32178775
- PMCID: PMC7113842
- DOI: 10.1016/S2213-2600(19)30469-2
Blood transcriptional biomarkers for active pulmonary tuberculosis in a high-burden setting: a prospective, observational, diagnostic accuracy study
Abstract
Background: Blood transcriptional signatures are candidates for non-sputum triage or confirmatory tests of tuberculosis. Prospective head-to-head comparisons of their diagnostic accuracy in real-world settings are necessary to assess their clinical use. We aimed to compare the diagnostic accuracy of candidate transcriptional signatures identified by systematic review, in a setting with a high burden of tuberculosis and HIV.
Methods: We did a prospective observational study nested within a diagnostic accuracy study of sputum Xpert MTB/RIF (Xpert) and Xpert MTB/RIF Ultra (Ultra) tests for pulmonary tuberculosis. We recruited consecutive symptomatic adults aged 18 years or older self-presenting to a tuberculosis clinic in Cape Town, South Africa. Participants provided blood for RNA sequencing, and sputum samples for liquid culture and molecular testing using Xpert and Ultra. We assessed the diagnostic accuracy of candidate blood transcriptional signatures for active tuberculosis (including those intended to distinguish active tuberculosis from other diseases) identified by systematic review, compared with culture or Xpert MTB/RIF positivity as the standard reference. In our primary analysis, patients with tuberculosis were defined as those with either a positive liquid culture or Xpert result. Patients with missing blood RNA or sputum results were excluded. Our primary objective was to benchmark the diagnostic accuracy of candidate transcriptional signatures against the WHO target product profile (TPP) for a tuberculosis triage test.
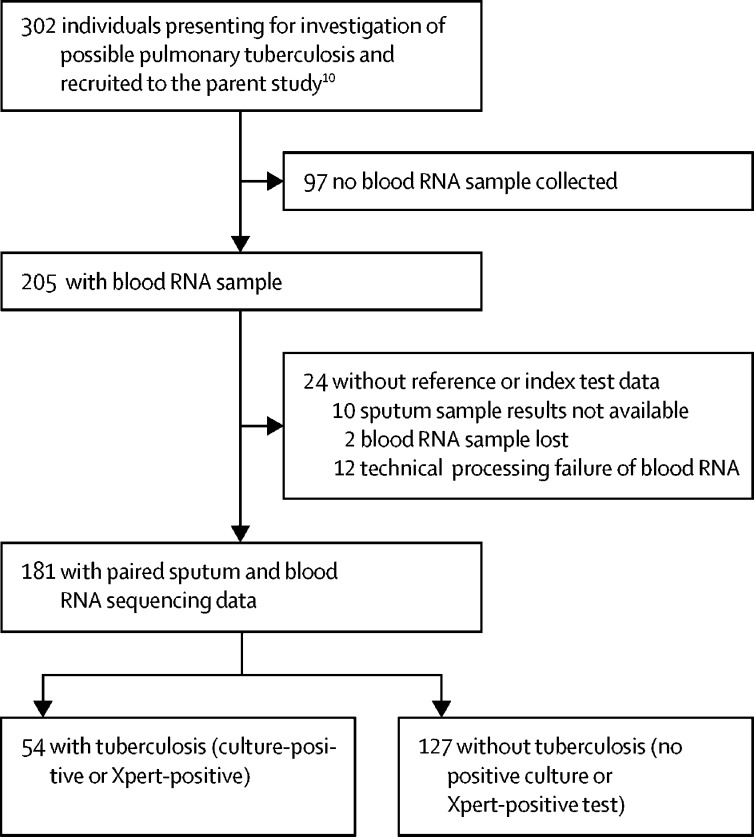
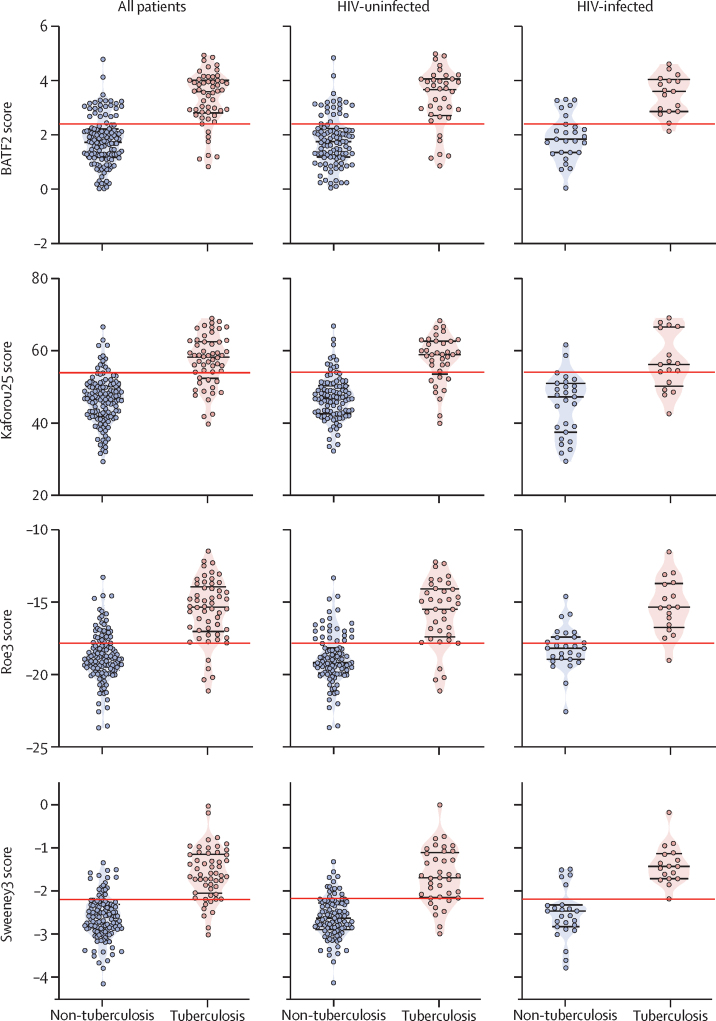
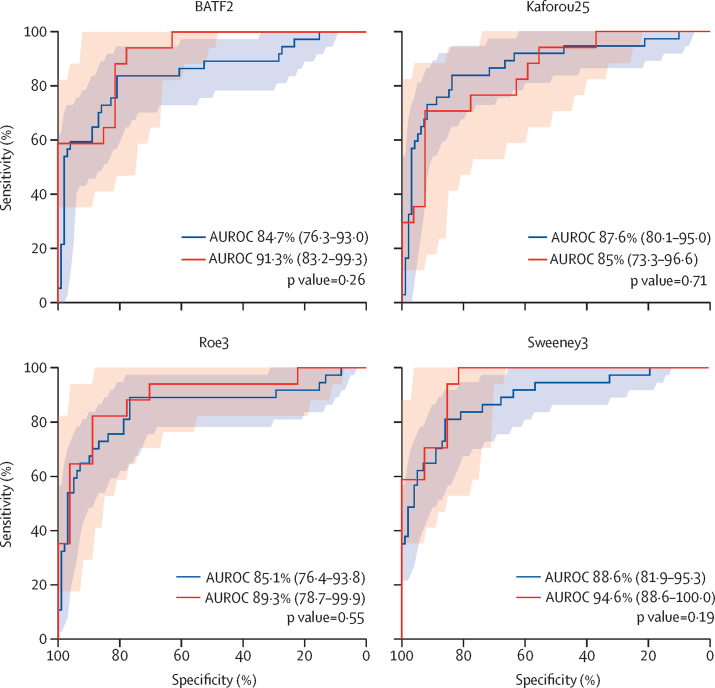
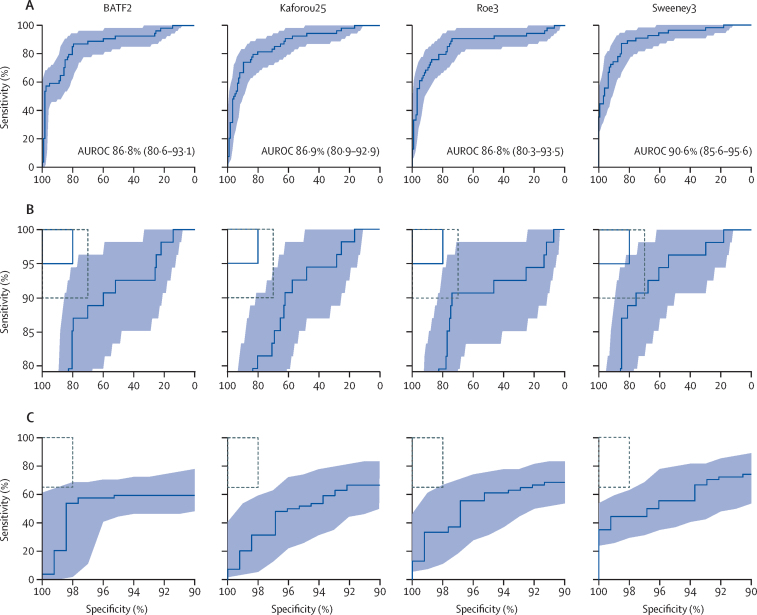
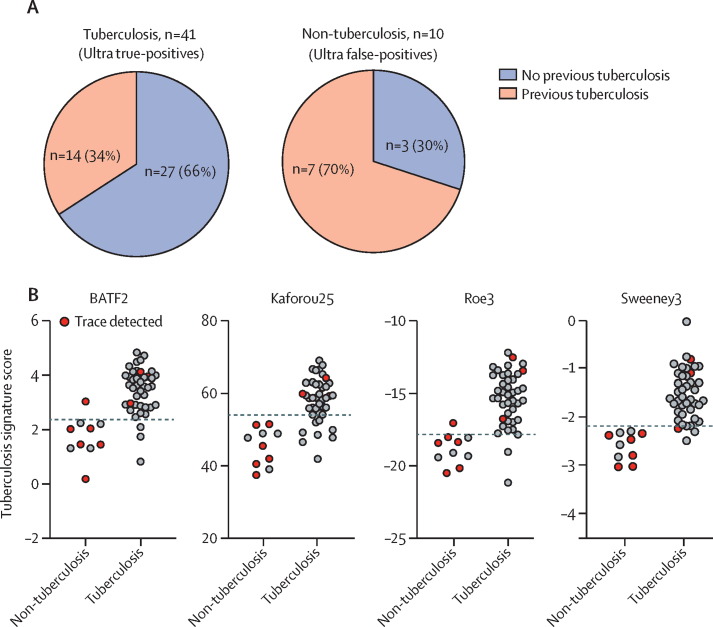
Findings: Between Feb 12, 2016, and July 18, 2017, we obtained paired sputum and RNA sequencing data from 181 participants, 54 (30%) of whom had confirmed pulmonary tuberculosis. Of 27 eligible signatures identified by systematic review, four achieved the highest diagnostic accuracy with similar area under the receiver operating characteristic curves (Sweeney3: 90·6% [95% CI 85·6-95·6]; Kaforou25: 86·9% [80·9-92·9]; Roe3: 86·9% [80·3-93·5]; and BATF2: 86·8% [80·6-93·1]), independent of age, sex, HIV status, previous tuberculosis, or sputum smear result. At test thresholds that gave 70% specificity (the minimum WHO TPP specificity for a triage test), these four signatures achieved sensitivities between 83·3% (95% CI 71·3-91·0) and 90·7% (80·1-96·0). No signature met the optimum criteria, of 95% sensitivity and 80% specificity proposed by WHO for a triage test, or the minimum criteria (of 65% sensitivity and 98% specificity) for a confirmatory test, but all four correctly identified Ultra-positive, culture-negative patients.
Interpretation: Selected blood transcriptional signatures met the minimum WHO benchmarks for a tuberculosis triage test but not for a confirmatory test. Further development of the signatures is warranted to investigate their possible effects on clinical and health economic outcomes as part of a triage strategy, or when used as add-on confirmatory test in conjunction with the highly sensitive Ultra test for Mycobacterium tuberculosis DNA.
Funding: Royal Society Newton Advanced Fellowship, Wellcome Trust, National Institute of Health Research, and UK Medical Research Council.
Copyright © 2020 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Blood transcriptional signatures for tuberculosis testing.Lancet Respir Med. 2020 Apr;8(4):330-331. doi: 10.1016/S2213-2600(20)30045-X. Epub 2020 Mar 13. Lancet Respir Med. 2020. PMID: 32178777 Free PMC article. No abstract available.
References
-
- WHO . World Health Organization; Geneva: 2019. Global tuberculosis report 2018.https://www.who.int/tb/publications/global_report/en/
-
- WHO . World Health Organization; Geneva: 2014. High-priority target product profiles for new tuberculosis diagnostics.https://www.who.int/tb/publications/tpp_report/en/
-
- MacLean E, Broger T, Yerlikaya S, Fernandez-Carballo BL, Pai M, Denkinger CM. A systematic review of biomarkers to detect active tuberculosis. Nat Microbiol. 2019;4:748–758. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
