

Microbial aetiology of brain abscess in a UK cohort: Prominent role of Streptococcus intermedius
- PMID: 32179070
- PMCID: PMC7267774
- DOI: 10.1016/j.jinf.2020.03.011
Microbial aetiology of brain abscess in a UK cohort: Prominent role of Streptococcus intermedius
Abstract
Background: Brain abscess is an uncommon condition, but carries high mortality. Current treatment guidelines are based on limited data. Surveillance of clinical, radiological and microbiology data is important to inform patient stratification, interventions, and antimicrobial stewardship.
Methods: We undertook a retrospective, observational study of patients with brain abscess, based on hospital coding, in a UK tertiary referral teaching hospital. We reviewed imaging data, laboratory microbiology, and antibiotic prescriptions.
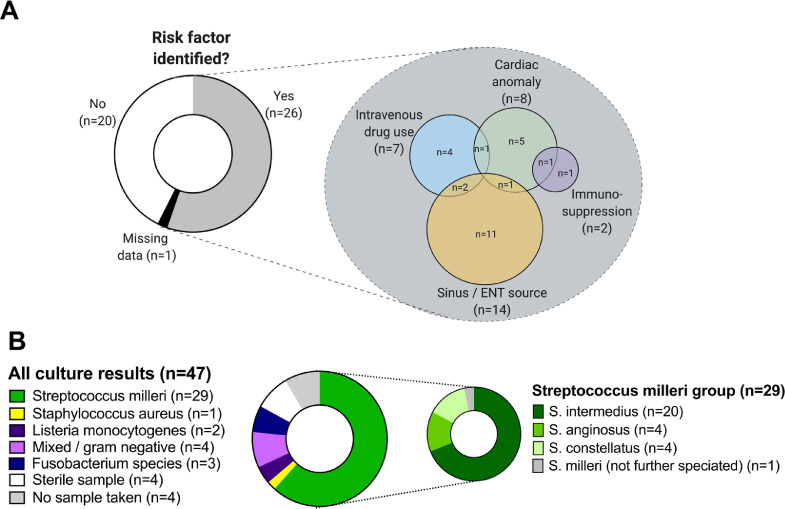
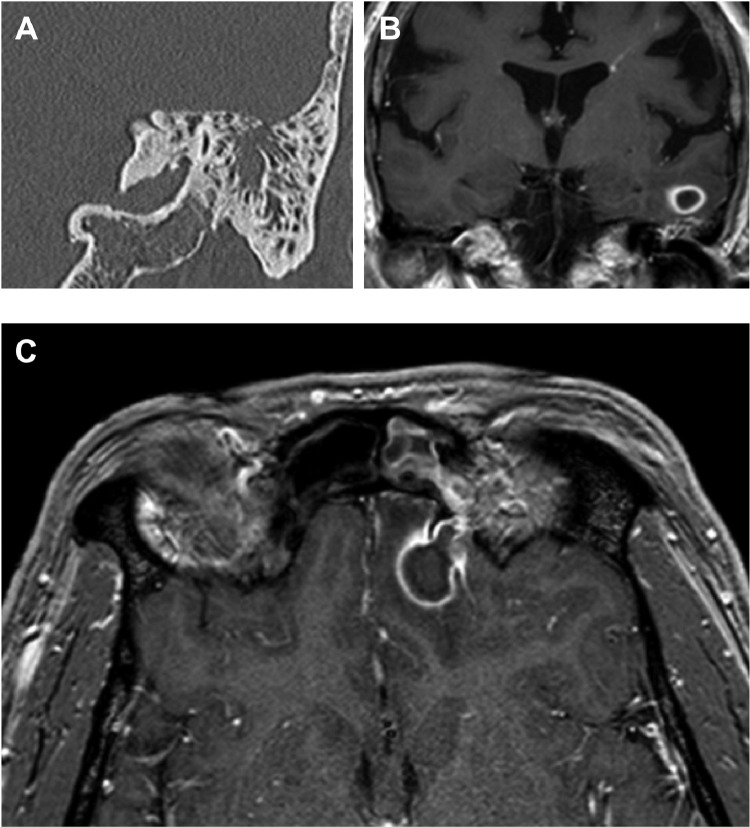
Results: Over a 47 month period, we identified 47 adults with bacterial brain abscess (77% male, median age 47 years). Most of the abscesses were solitary frontal or parietal lesions. A microbiological diagnosis was secured in 39/47 (83%) of cases, among which the majority were of the Streptococcus milleri group (27/39; 69%), with a predominance of Streptococcus intermedius (19/27; 70%). Patients received a median of 6 weeks of intravenous antibiotics (most commonly ceftriaxone), with variable oral follow-on regimens. Ten patients (21%) died, up to 146 days after diagnosis. Mortality was significantly associated with increasing age, multiple abscesses, immunosuppression and the presence of an underlying cardiac anomaly.
Conclusion: Our data suggest that there has been a shift away from staphylococcal brain abscesses, towards S. intermedius as a dominant pathogen. In our setting, empiric current first line therapy with ceftriaxone remains appropriate on microbiological grounds and narrower spectrum therapy may sometimes be justified. Mortality of this condition remains high among patients with comorbidity. Prospective studies are required to inform optimum dose, route and duration of antimicrobial therapy.
Keywords: Aetiology; Brain abscess; Epidemiology; Imaging, antibiotics; Microbiology; Prevalence; Streptococci; Streptococcus milleri.
Copyright © 2020. Published by Elsevier Ltd.
Figures
References
-
- Brouwer M.C., Tunkel A.R., McKhann G.M., van de Beek D. Brain abscess. Nejm. 2014;371(5):447–456. - PubMed
-
- Tandon S., Beasley N., Swift A.C. Changing trends in intracranial abscesses secondary to ear and sinus disease. J Laryngol Otol. 2009 Mar 19;123(03):283. - PubMed
-
- Brouwer M.C., van de Beek D. Epidemiology, diagnosis, and treatment of brain abscesses. Curr Opin Infect Dis. 2016 Nov;30(1):129–134. - PubMed
-
- Sonneville R., Ruimy R., Benzonana N., Riffaud L., Carsin A., Tadié J.-.M. An update on bacterial brain abscess in immunocompetent patients. Clin Microbiol Infect. 2017 Sep;23(9):614–620. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
