

Combination of PD-1 Inhibitor and OX40 Agonist Induces Tumor Rejection and Immune Memory in Mouse Models of Pancreatic Cancer
- PMID: 32179091
- PMCID: PMC7387152
- DOI: 10.1053/j.gastro.2020.03.018
Combination of PD-1 Inhibitor and OX40 Agonist Induces Tumor Rejection and Immune Memory in Mouse Models of Pancreatic Cancer
Abstract
Background & aims: Advanced pancreatic ductal adenocarcinoma (PDAC) is resistant to therapy, including immune checkpoint inhibitors. We evaluated the effects of a neutralizing antibody against programmed cell death 1 (PD-1) and an agonist of OX40 (provides a survival signal to activated T cells) in mice with pancreatic tumors.
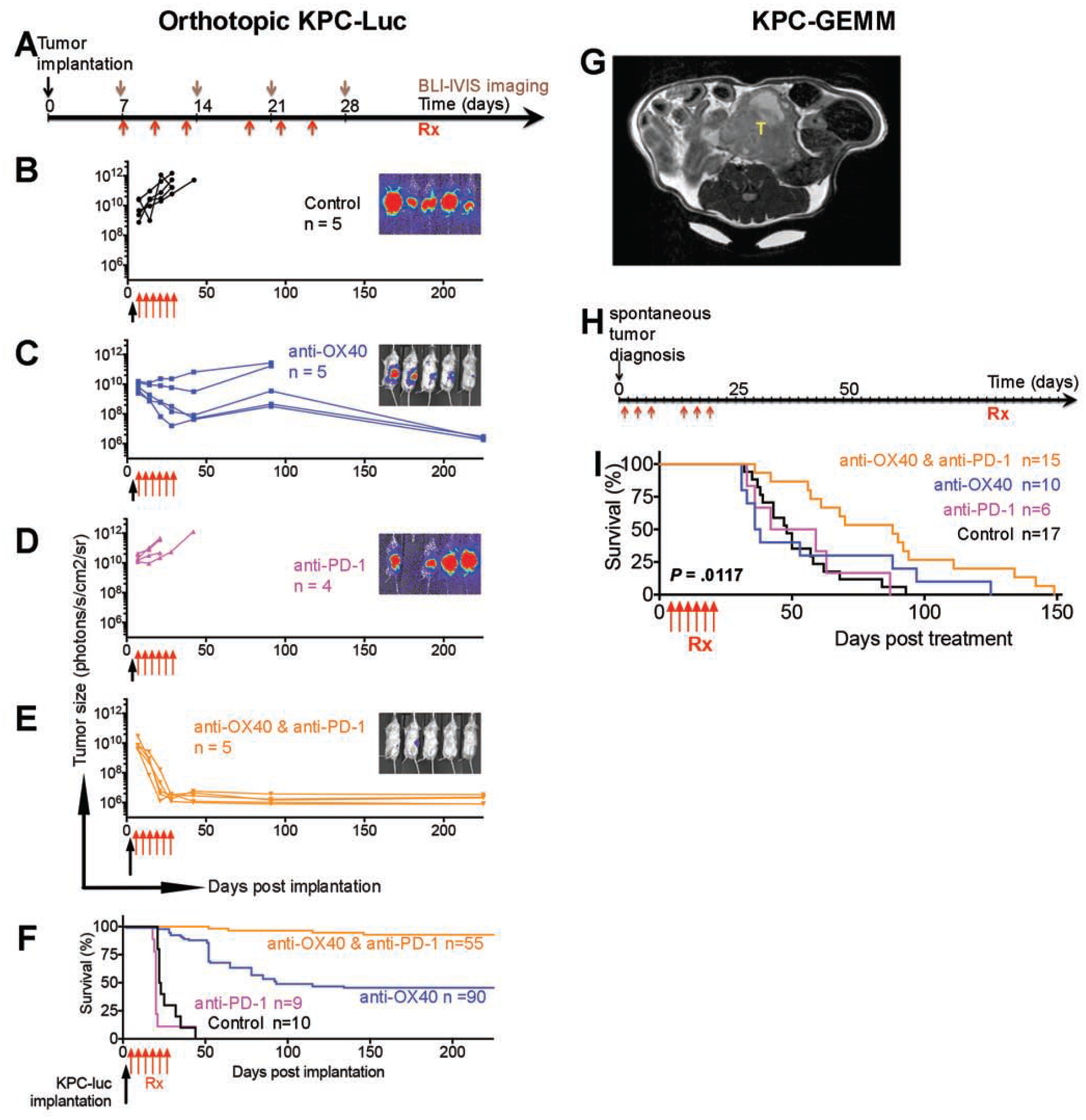
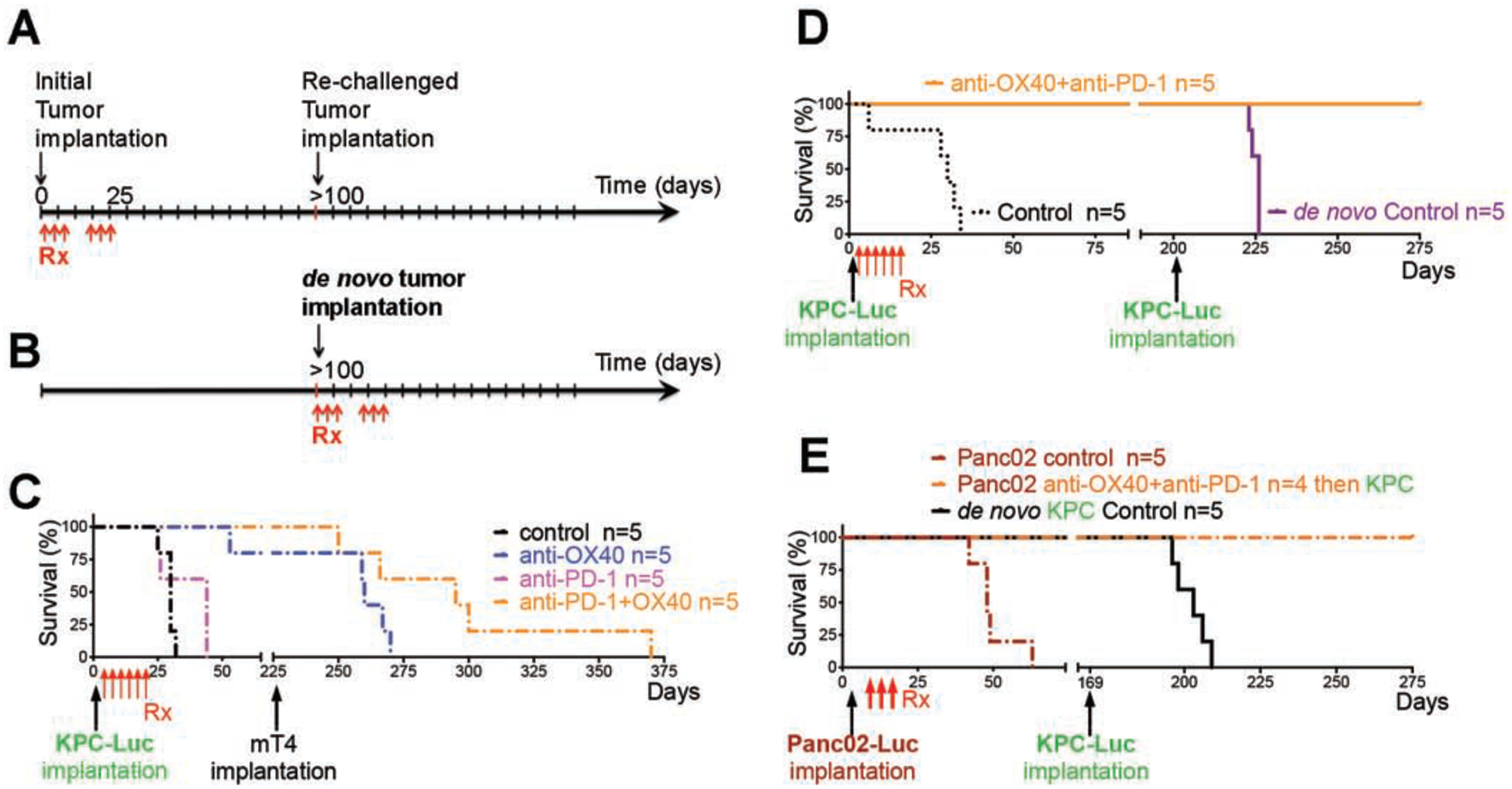
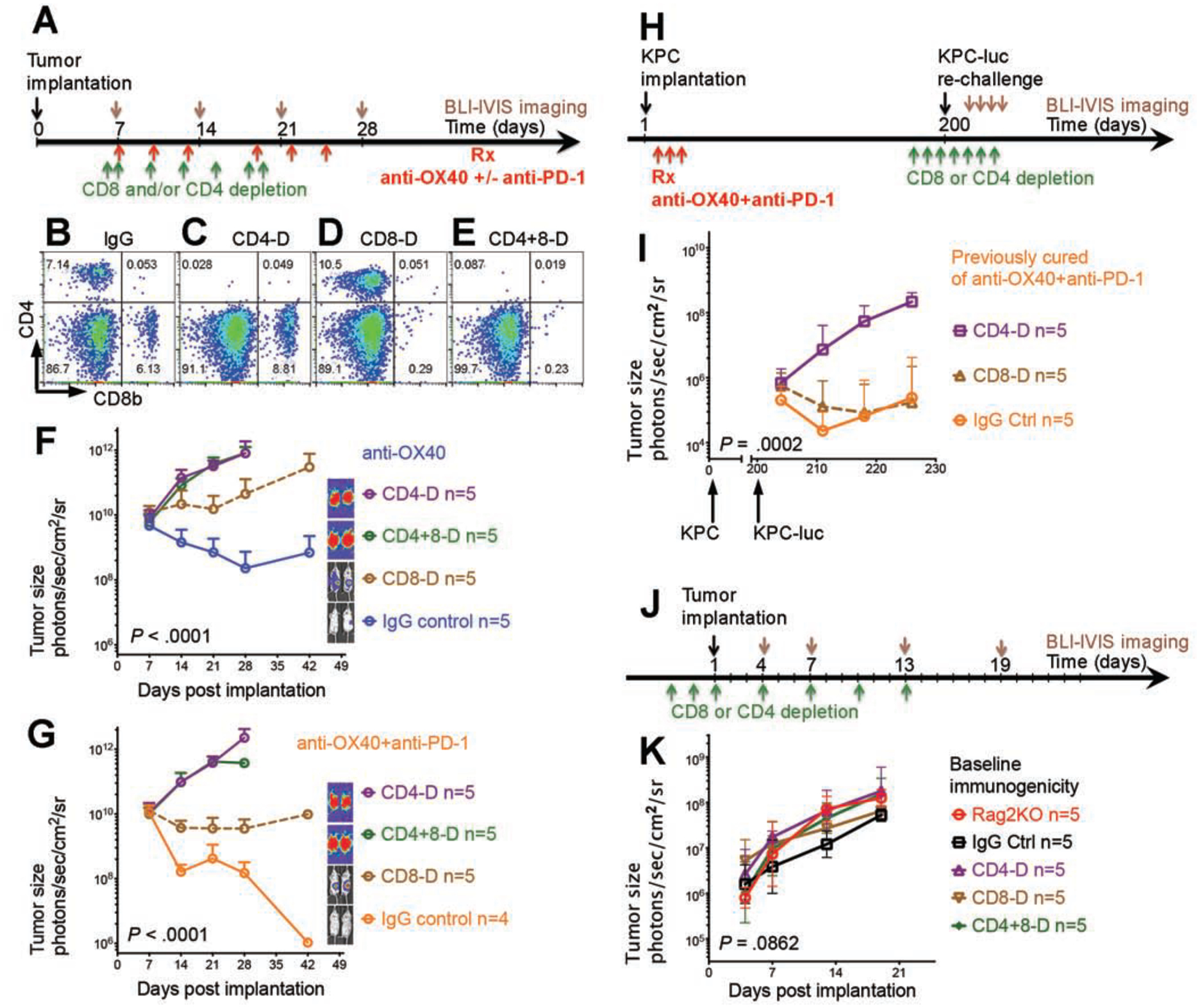
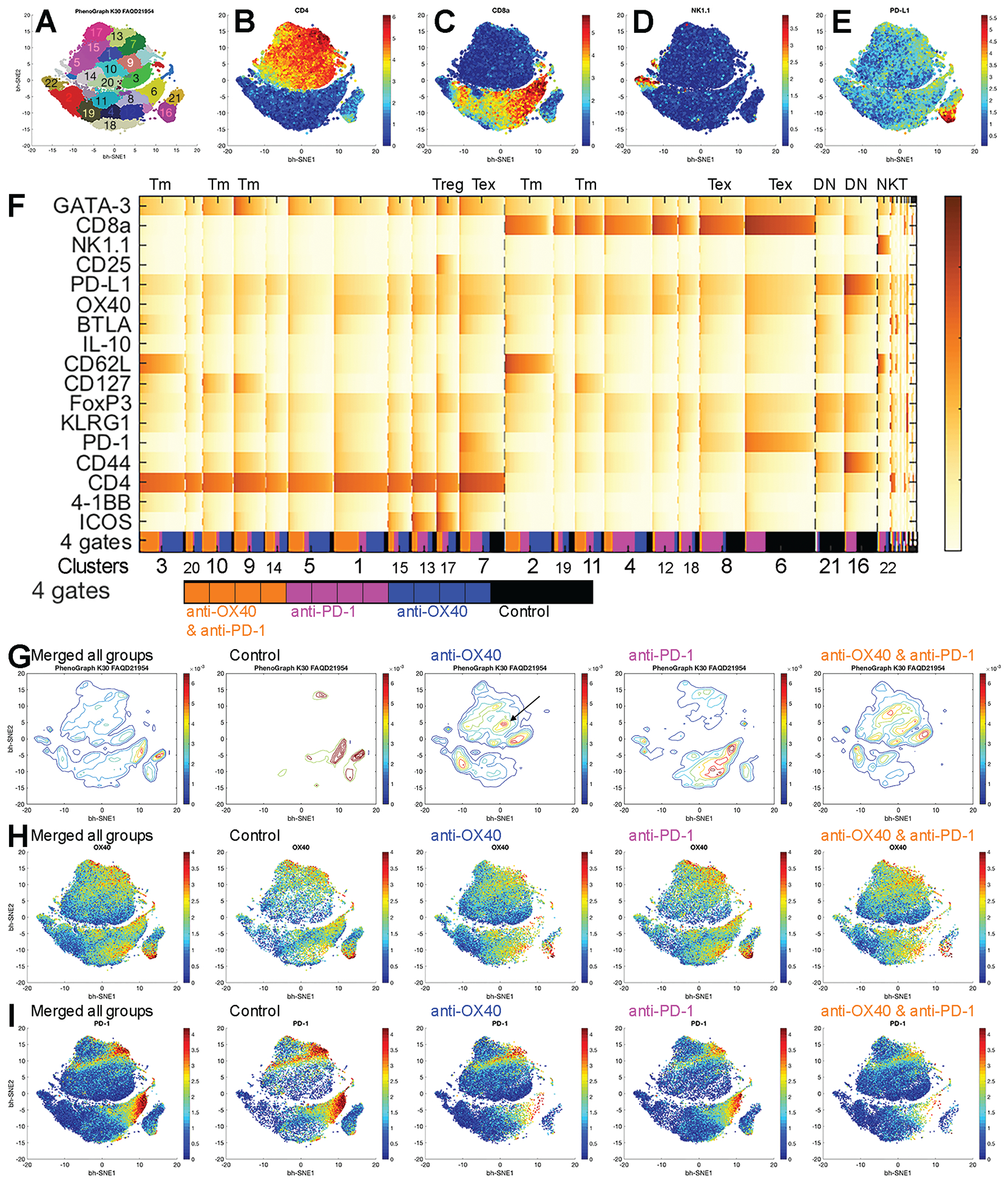
Methods: We performed studies in C57BL/6 mice (controls), KrasG12D/+;Trp53R172H/+;Pdx-1-Cre (KPC) mice, and mice with orthotopic tumors grown from Panc02 cells, KrasG12D;P53flox/flox;PDX-1-Cre;Luciferase (KPC-Luc) cells, or mT4 cells. After tumors developed, mice were given injections of control antibody or anti-OX40 and/or anti-PD-1 antibody. Some mice were then given injections of antibodies against CD8, CD4, or NK1.1 to deplete immune cells, and IL4 or IL7RA to block cytokine signaling. Bioluminescence imaging was used to monitor tumor growth. Tumor tissues collected and single-cell suspensions were analyzed by time of flight mass spectrometry analysis. Mice that were tumor-free 100 days after implantation of orthotopic tumors were rechallenged with PDAC cells (KPC-Luc or mT4) and survival was measured. Median levels of PD-1 and OX40 mRNAs in PDACs were determined from The Cancer Genome Atlas and compared with patient survival times.
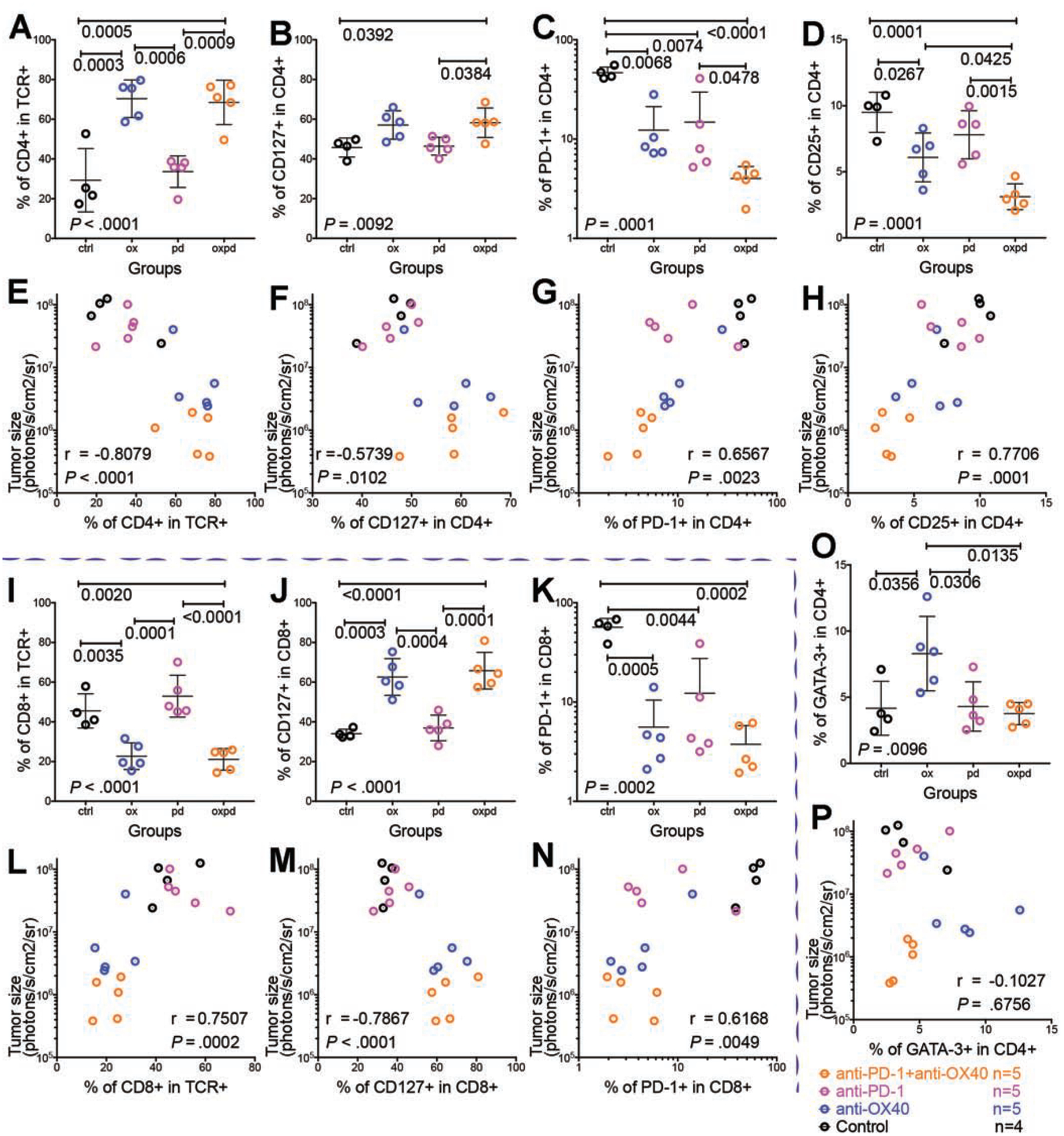
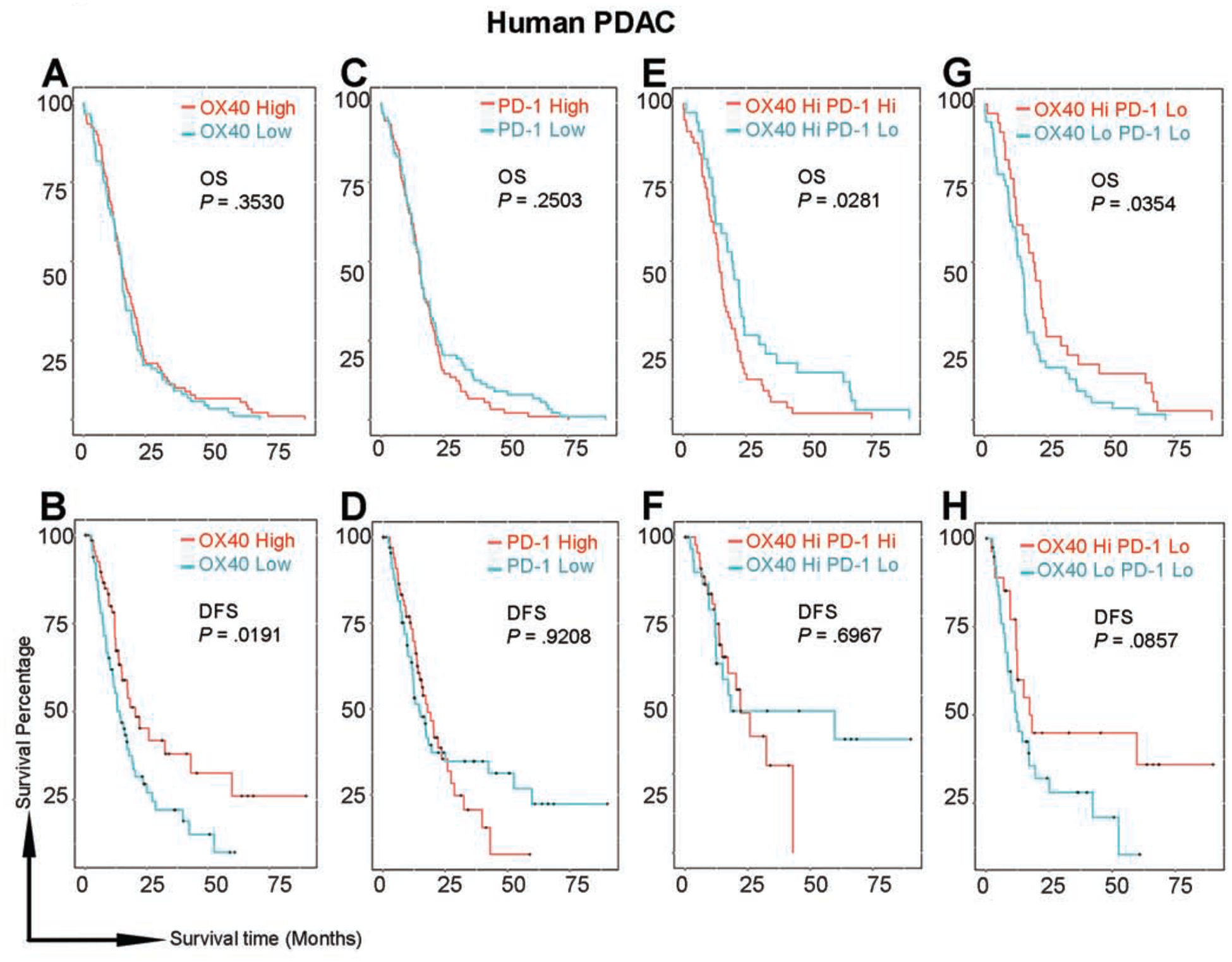
Results: In mice with orthotopic tumors, all those given control antibody or anti-PD-1 died within 50 days, whereas 43% of mice given anti-OX40 survived for 225 days; almost 100% of mice given the combination of anti-PD-1 and anti-OX40 survived for 225 days, and tumors were no longer detected. KPC mice given control antibody, anti-PD-1, or anti-OX40 had median survival times of 50 days or less, whereas mice given the combination of anti-PD-1 and anti-OX40 survived for a median 88 days. Mice with orthotopic tumors that were given the combination of anti-PD-1 and anti-OX40 and survived 100 days were rechallenged with a second tumor; those rechallenged with mT4 cells survived an additional median 70 days and those rechallenged with KPC-Luc cells survived long term, tumor free. The combination of anti-PD-1 and anti-OX40 did not slow tumor growth in mice with antibody-mediated depletion of CD4+ T cells. Mice with orthotopic tumors given the combination of anti-PD-1 and anti-OX40 that survived after complete tumor rejection were rechallenged with KPC-Luc cells; those with depletion of CD4+ T cells before the rechallenge had uncontrolled tumor growth. Furthermore, KPC orthotopic tumors from mice given the combination contained an increased number of CD4+ T cells that expressed CD127 compared with mice given control antibody. The combination of agents reduced the proportion of T-regulatory and exhausted T cells and decreased T-cell expression of GATA3; tumor size was negatively associated with numbers of infiltrating CD4+ T cells, CD4+CD127+ T cells, and CD8+CD127+ T cells, and positively associated with numbers of CD4+PD-1+ T cells, CD4+CD25+ T cells, and CD8+PD-1+ T cells. PDACs with high levels of OX40 and low levels of PD-1 were associated with longer survival times of patients.
Conclusions: Pancreatic tumors appear to evade the immune response by inducing development of immune-suppressive T cells. In mice, the combination of anti-PD-1 inhibitory and anti-OX40 agonist antibodies reduces the proportion of T-regulatory and exhausted T cells in pancreatic tumors and increases numbers of memory CD4+ and CD8+ T cells, eradicating all detectable tumor. This information can be used in development of immune-based combination therapies for PDAC.
Keywords: CyTOF; Immune Checkpoint Inhibitor; Immune-Based Therapy; Mouse Model.
Copyright © 2020 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Clark CE, Hingorani SR, Mick R, et al. Dynamics of the immune reaction to pancreatic cancer from inception to invasion. Cancer Res 2007;67:9518–27. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
