

Role of advanced left ventricular imaging in adults with aortic stenosis
- PMID: 32179586
- PMCID: PMC7306876
- DOI: 10.1136/heartjnl-2019-315211
Role of advanced left ventricular imaging in adults with aortic stenosis
Abstract
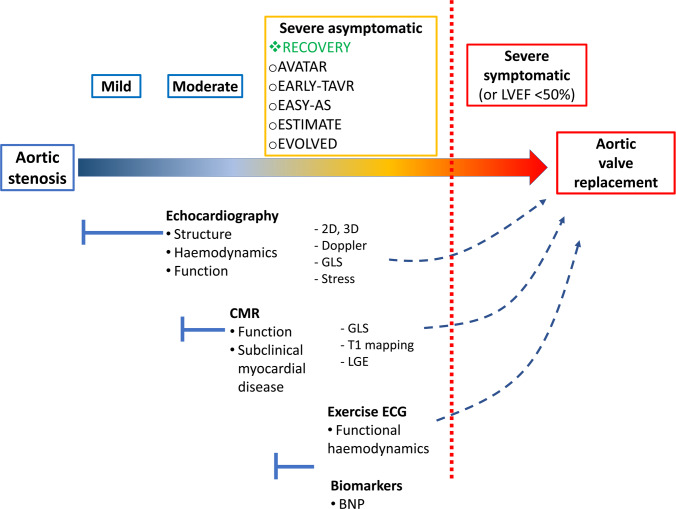
This review focuses on the available data regarding the utility of advanced left ventricular (LV) imaging in aortic stenosis (AS) and its potential impact for optimising the timing of aortic valve replacement. Ejection fraction is currently the only LV parameter recommended to guide intervention in AS. The cut-off value of 50%, recommended for decision-making in asymptomatic patients with AS, is currently under debate. Several imaging parameters have emerged as predictors of disease progression and clinical outcomes in this setting. Global longitudinal LV strain by speckle tracking echocardiography is useful for risk stratification of asymptomatic patients with severe AS and preserved LV ejection fraction. Its prognostic value was demonstrated in these patients, but further work is required to define the best thresholds to aid the decision-making process. The assessment of myocardial fibrosis is the most studied application of cardiac magnetic resonance in AS. The detection of replacement fibrosis by late gadolinium enhancement offers incremental prognostic information in these patients. Clinical implementation of this technique to optimise the timing of aortic valve intervention in asymptomatic patients is currently tested in a randomised trial. The use of T1 mapping techniques can provide an assessment of interstitial myocardial fibrosis and represents an expanding field of interest. However, convincing data in patients with AS is still lacking. All these imaging parameters have substantial potential to influence the management decision in patients with AS in the future, but data from randomised clinical trials are awaited to define their utility in daily practice.
Keywords: advanced cardiac imaging; aortic stenosis; cardiac magnetic resonance (CMR) imaging; echocardiography.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: BAP has received research support and lecture honoraria from General Electric Healthcare.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials