

Myocardial Minimal Damage After Rapid Ventricular Pacing - the prospective randomized multicentre MyDate-Trial
- PMID: 32179792
- PMCID: PMC7075963
- DOI: 10.1038/s41598-020-61625-8
Myocardial Minimal Damage After Rapid Ventricular Pacing - the prospective randomized multicentre MyDate-Trial
Abstract
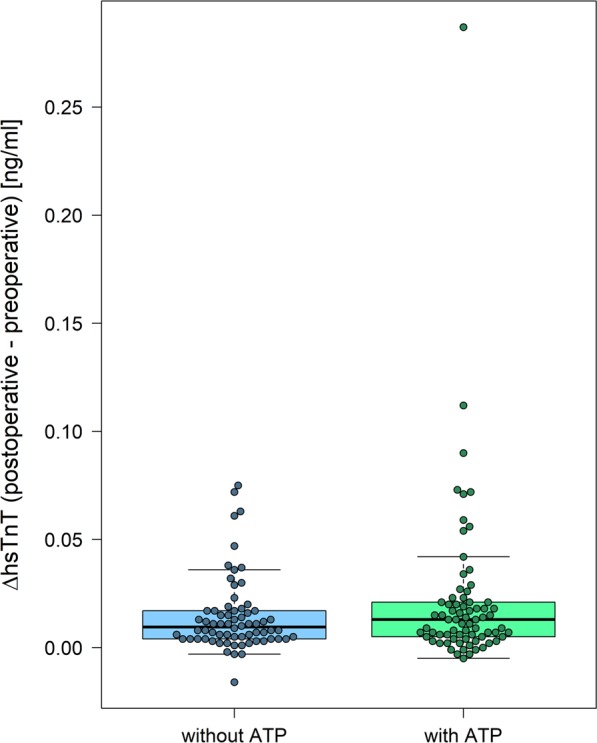
Therapy of choice for the primary and secondary prevention of sudden cardiac death is the implantation of an implantable cardioverter defibrillator (ICD). Whereas appropriate and inappropriate ICD shocks lead to myocardial microdamage, this is not known for antitachycardia pacing (ATP). In total, 150 ICD recipients (66 ± 12 years, 81.3% male, 93.3% primary prevention, 30.0% resynchronization therapy) were randomly assigned to an ICD implantation with or without intraoperative ATP. In the group with ATP, the pacing maneuver was performed twice, each time applying 8 impulses à 6 Volt x 1.0 milliseconds to the myocardium. High sensitive Troponin T (hsTnT) levels were determined prior to the implantation and thereafter. There was no significant difference in the release of hsTnT between the two randomization groups (delta TnT without ATP in median 0.010 ng/ml [min. -0.016 ng/ml-max. 0.075 ng/ml] vs. with ATP in median 0.013 ng/ml [min. -0.005-0.287 ng/ml], p = 0.323). Setting a hsTnT cutoff of 0.059 ng/dl as a regularly augmented postoperative hsTnT level, no relevant difference between the two groups regarding the postoperative hsTnT levels above this cutoff could be identified (without ATP n = 10 [14.7%] vs. with ATP n = 16 [21.9%], p = 0.287). There was no significant difference in the release of high sensitive Troponin between patients without intraoperative ATP compared to those with intraoperative ATP. Hence, antitachycardia pacing does not seem to cause significant myocardial microdamage. This may further support its use as a painless and efficient method to terminate ventricular tachycardia in high-risk patients.
Conflict of interest statement
V.S. received travel support from Sorin Group and Abbott Medical. She received educational grants and training from Abbott Medical (St. Jude Medical) and Boston Scientific. P.B. received travel support from Abbott Medical and lecture honoraria from Biotronik. S.W. reports lecture honoraria from German Cardiac Society (DGK); he has received educational grants and training from Abbott Medical (St. Jude Medical) and Biotronik. M.K. reports lecture honoraria from Bristol-Myers Squibb and Bayer. C.K. reports speaker fees/travel support from Abbott Medical, Biotronik, Boston Scientific, Bristol-Myers-Squibb, Microport, Novartis, Philips; he has participated in clinical studies supported by Abbott Medical, Biotronik, Boston Scientific, Microport and is/has been an advisor to Biotronik and Microport. C.D., B.H., C.L., A.B., C.G. and S.B. declare no conflicts of interests.
Figures


References
-
- Wathen MS, et al. Prospective randomized multicenter trial of empirical antitachycardia pacing versus shocks for spontaneous rapid ventricular tachycardia in patients with implantable cardioverter-defibrillators. Pacing fast ventricular tachycardia reduces shock therapies (PainFREE Rx II) Trial Results. Circulation. 2004;110:2591–2596. doi: 10.1161/01.CIR.0000145610.64014.E4. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
