

Quantitative coronary computed tomography angiography for the detection of cardiac allograft vasculopathy
- PMID: 32179995
- PMCID: PMC7338811
- DOI: 10.1007/s00330-019-06653-3
Quantitative coronary computed tomography angiography for the detection of cardiac allograft vasculopathy
Abstract
Objectives: To associate coronary wall volume and composition, derived from coronary computed tomography angiography (CTA), with cardiac allograft vasculopathy (CAV) detected on invasive coronary angiography (ICA) in heart-transplanted (HTX) patients.
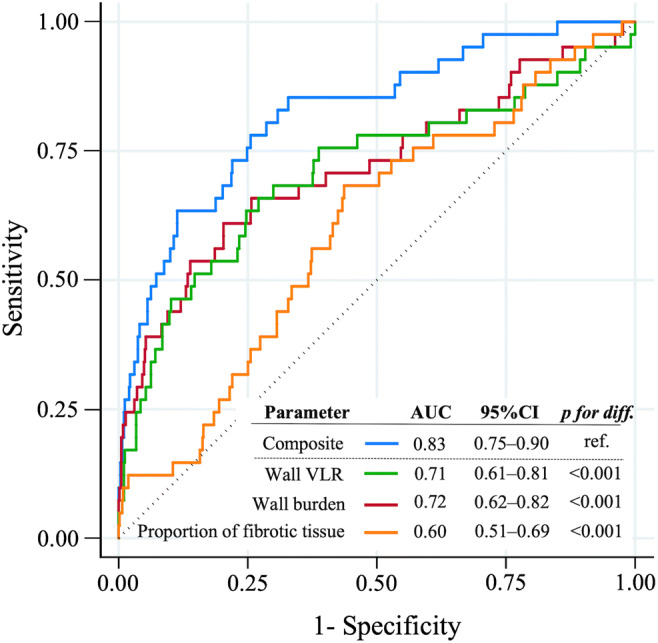
Methods: We included consecutive adults who received ICA and coronary CTA for evaluation of CAV ≥ 10 months after HTX. In all coronary segments, we assessed lumen and wall volumes and segmental length, calculated volume-length ratio (VLR) (volumes indexed by segmental length; mm3/mm), wall burden (WB) (wall/wall + lumen volumes; %), and assessed proportions of calcified, fibrotic, fibro-fatty, and low-attenuation tissue (%) in coronary wall. We rendered independent CTA measures associated with CAV by ICA, tested their discriminatory capacity, and assessed concordance between CTA and ICA.
Results: Among 50 patients (84% men; 53.6 ± 11.9 years), we analyzed 632 coronary segments. Mean interval between HTX and CTA was 6.7 ± 4.7 years and between ICA and CTA 1 (0-1) day. Segmental VLR, WB, and proportion of fibrotic tissue were independently associated with CAV (OR = 1.06-1.27; p ≤ 0.002), reaching a high discriminatory capacity (combination of all three: AUC = 0.84; 95%CI, 0.75-0.90). Concordance between CTA and ICA was higher in advanced CAV (88%) compared with that in none (37%) and mild (19%) CAV. Discordance was primarily driven by a large number of segments with coronary wall changes on CTA but without luminal stenoses on ICA (177/591; 25%).
Conclusion: CTA-derived coronary wall VLR, WB, and the proportion of fibrotic tissue are independent markers of CAV. Combination of these three parameters may aid the detection of early CAV not detected by ICA, the current standard of care.
Key points: • Coronary CTA detects CAV in HTX patients. • Coronary wall volume-length ratio, wall burden, and proportion of fibrotic tissue are independently associated with CAV. • In contrast to ICA, coronary CTA may identify the early stages of CAV.
Keywords: Cardiac allograft vasculopathy; Computed tomography angiography; Heart transplantation; Invasive coronary angiography.
Conflict of interest statement
The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article.
Figures

Similar articles
-
Coronary computed tomography in heart transplant patients: detection of significant stenosis and cardiac allograft vasculopathy, image quality, and radiation dose.Acta Radiol. 2018 Sep;59(9):1066-1073. doi: 10.1177/0284185117748354. Epub 2017 Dec 20. Acta Radiol. 2018. PMID: 29260577
-
Quantitative CT assessment identifies more heart transplanted patients with progressive coronary wall thickening than standard clinical read.J Cardiovasc Comput Tomogr. 2019 Mar-Apr;13(2):128-133. doi: 10.1016/j.jcct.2018.11.006. Epub 2018 Nov 19. J Cardiovasc Comput Tomogr. 2019. PMID: 30528167
-
Comprehensive Non-invasive Versus Invasive Approach to Evaluate Cardiac Allograft Vasculopathy in Heart Transplantation: The CCTA-HTx Study.Circ Cardiovasc Imaging. 2025 Jan;18(1):e017197. doi: 10.1161/CIRCIMAGING.124.017197. Epub 2025 Jan 7. Circ Cardiovasc Imaging. 2025. PMID: 39764680
-
European Association of Cardiovascular Imaging/Cardiovascular Imaging Department of the Brazilian Society of Cardiology recommendations for the use of cardiac imaging to assess and follow patients after heart transplantation.Eur Heart J Cardiovasc Imaging. 2015 Sep;16(9):919-48. doi: 10.1093/ehjci/jev139. Epub 2015 Jul 2. Eur Heart J Cardiovasc Imaging. 2015. PMID: 26139361 Review.
-
Coronary computed tomography angiography for the detection of cardiac allograft vasculopathy: a meta-analysis of prospective trials.J Am Coll Cardiol. 2014 May 20;63(19):1992-2004. doi: 10.1016/j.jacc.2014.01.071. Epub 2014 Mar 26. J Am Coll Cardiol. 2014. PMID: 24681148
Cited by
-
Epicardial fat volume is related to the degree of cardiac allograft vasculopathy.Eur Radiol. 2023 Jan;33(1):330-338. doi: 10.1007/s00330-022-09029-2. Epub 2022 Aug 20. Eur Radiol. 2023. PMID: 35986769 Free PMC article.
-
Thickness and Volume of Epicardial Adipose Tissue in Relation to Stiffness and Elasticity of Aorta Assessed by Computed Tomography Angiography.Biomedicines. 2023 Jun 1;11(6):1617. doi: 10.3390/biomedicines11061617. Biomedicines. 2023. PMID: 37371711 Free PMC article.
-
Revisiting Biomarkers of Cardiac Allograft Vasculopathy: Addressing the Achilles Heel of Heart Transplantation.Curr Heart Fail Rep. 2024 Dec;21(6):580-590. doi: 10.1007/s11897-024-00685-7. Epub 2024 Oct 17. Curr Heart Fail Rep. 2024. PMID: 39414739 Review.
-
Clinical implementation of coronary computed tomography angiography for routine detection of cardiac allograft vasculopathy in heart transplant patients.Transpl Int. 2021 Oct;34(10):1886-1894. doi: 10.1111/tri.13973. Epub 2021 Sep 19. Transpl Int. 2021. PMID: 34268796 Free PMC article.
-
Successful treatment of rejection-related atrial tachycardia with pulse steroid after heart transplantation.Anatol J Cardiol. 2021 Mar;25(3):205-208. doi: 10.14744/AnatolJCardiol.2020.64859. Anatol J Cardiol. 2021. PMID: 33690136 Free PMC article. No abstract available.
References
-
- Lund LH, Edwards LB, Kucheryavaya AY, et al. The registry of the International Society for Heart and Lung Transplantation: thirty-second official adult heart transplantation report—2015; focus theme: early graft failure. J Heart Lung Transplant. 2015;34:1244–1254. doi: 10.1016/j.healun.2015.08.003. - DOI - PubMed
-
- Badano LP, Miglioranza MH, Edvardsen T, et al. European Association of Cardiovascular Imaging/Cardiovascular Imaging Department of the Brazilian Society of Cardiology recommendations for the use of cardiac imaging to assess and follow patients after heart transplantation. Eur Heart J Cardiovasc Imaging. 2015;16:919–948. doi: 10.1093/ehjci/jev139. - DOI - PubMed
-
- Costanzo MR, Dipchand A, Starling R et al (2010) The International Society of Heart and Lung Transplantation Guidelines for the care of heart transplant recipients. J Heart Lung Transplant 29:914–956. 10.1016/j.healun.2010.05.034 - PubMed
-
- Chih S, Chong AY, Mielniczuk LM, Bhatt DL, Beanlands RS (2016) Allograft vasculopathy: the Achilles’ heel of heart transplantation. J Am Coll Cardiol 68:80–91. 10.1016/j.jacc.2016.04.033 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
