

A plan template-based automation solution using a commercial treatment planning system
- PMID: 32180351
- PMCID: PMC7286016
- DOI: 10.1002/acm2.12848
A plan template-based automation solution using a commercial treatment planning system
Abstract
Purpose: The purpose of this study was to develop an auto-planning platform to be interfaced with a commercial treatment planning system (TPS). The main goal was to obtain robust and high-quality plans for different anatomic sites and various dosimetric requirements.
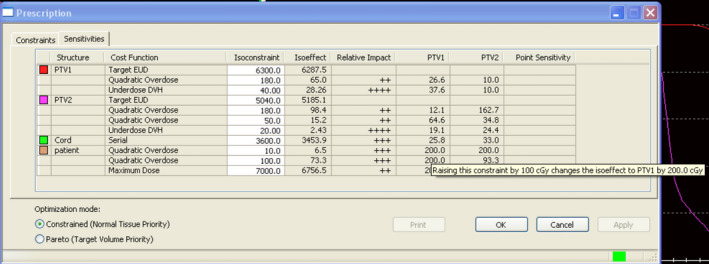
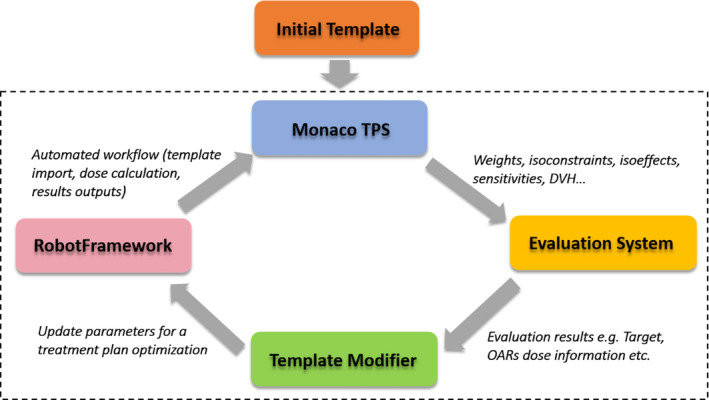
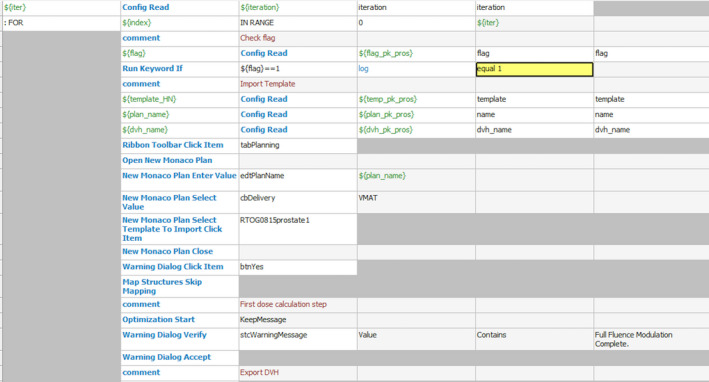
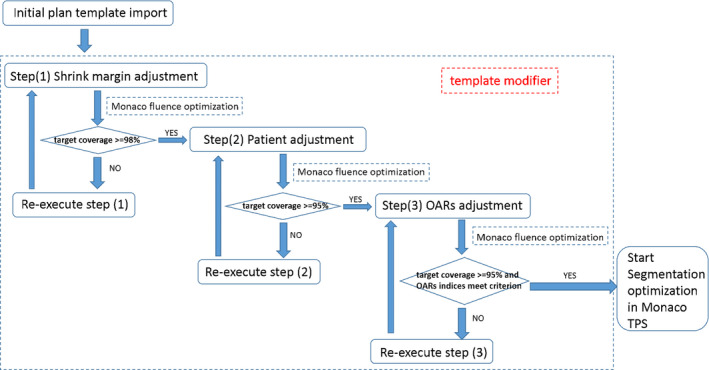
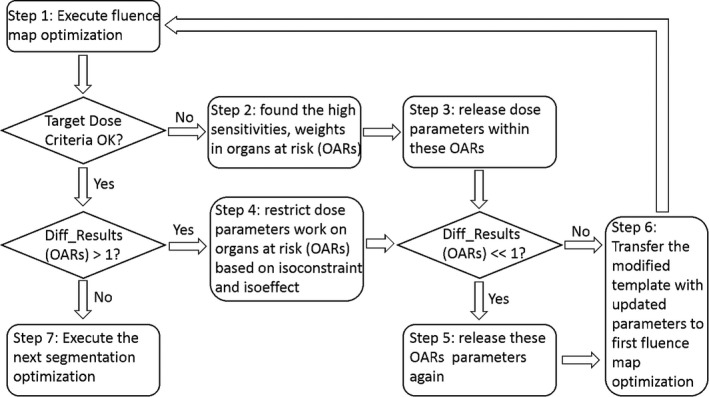
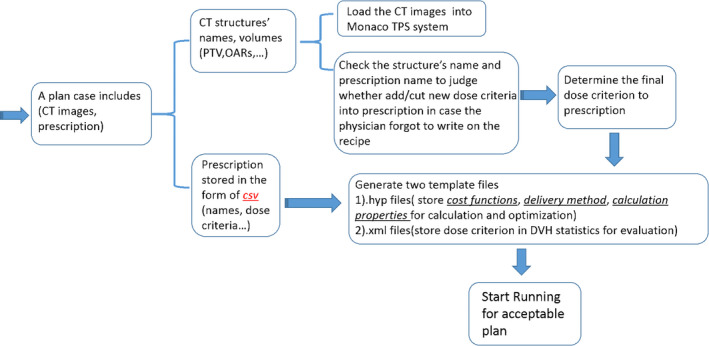
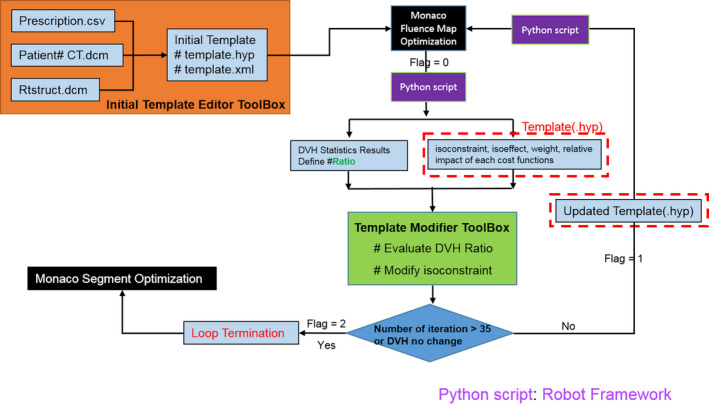
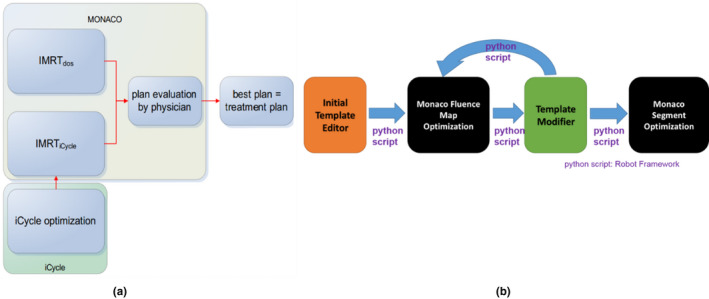
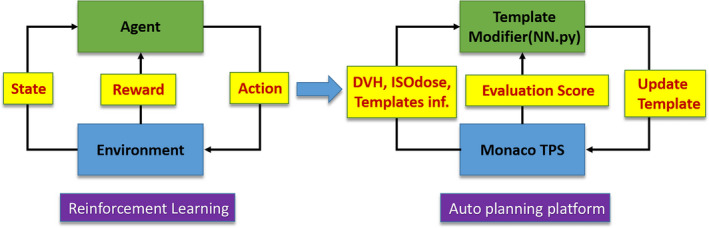
Methods: Monaco (Elekta, St. Louis, US) was the TPS in this work. All input parameters for inverse planning could be defined in a plan template inside Monaco. A software tool called Robot Framework was used to launch auto-planning trials with updated plan templates. The template modifier external to Monaco was the major component of our auto-planning platform. For current implementation, it was a rule-based system that mimics the trial-and-error process of an experienced planner. A template was automatically updated by changing the optimization constraints based on dosimetric evaluation of the plan obtained in the previous trial, along with the data of the iterative optimization extracted from Monaco. Treatment plans generated by Monaco with all plan evaluation criteria satisfied were considered acceptable, and such plans would be saved for further evaluation by clinicians. The auto-planning platform was validated for 10 prostate and 10 head-and-neck cases in comparison with clinical plans generated by experienced planners.
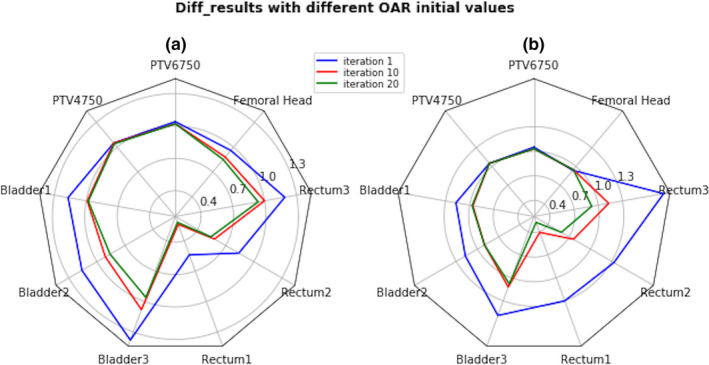
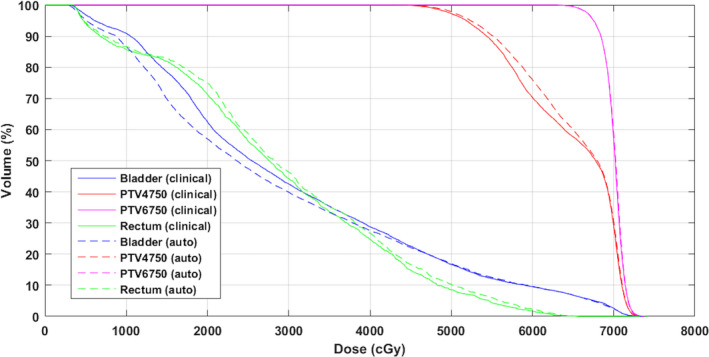
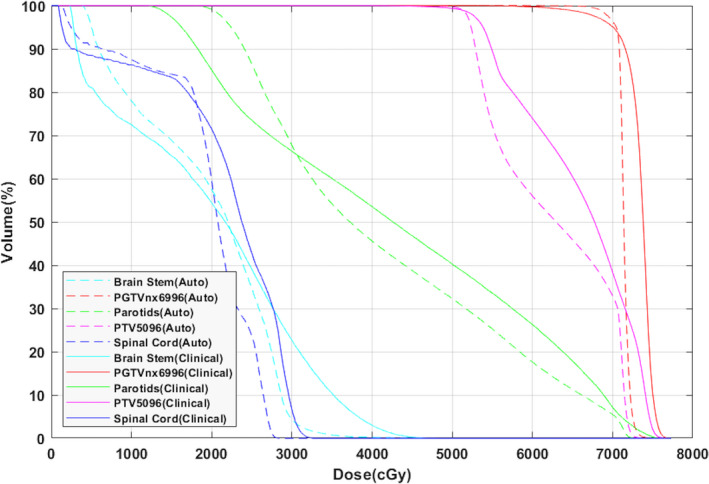
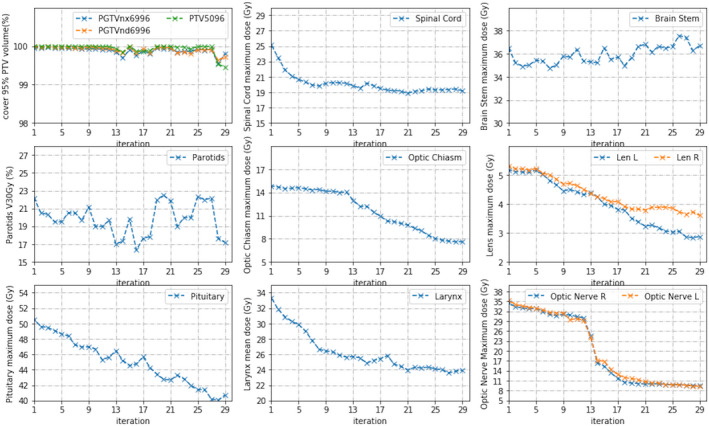
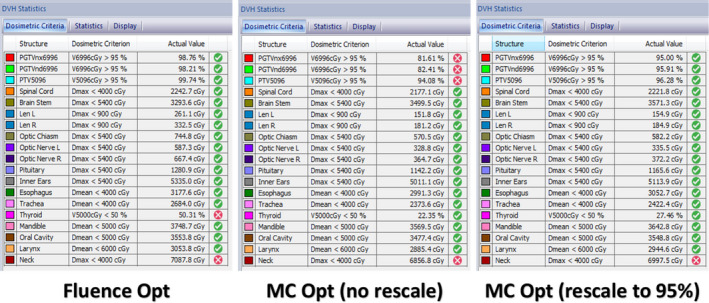
Results: The performance and robustness of our auto-planning platform was tested with clinical cases of prostate and head and neck treatment. For prostate cases, automatically generated plans had very similar plan quality with the clinical plans, and the bladder volume receiving 62.5 Gy, 50 Gy, and 40 Gy in auto-plans was reduced by 1%, 3%, and 5%, respectively. For head and neck cases, auto-plans had better conformity with reduced dose to the normal structures but slightly higher dose inhomogeneity in the target volume. Remarkably, the maximum dose in the spinal cord and brain stem was reduced by more than 3.5 Gy in auto-plans. Fluence map optimization only with less than 30 trials was adequate to generate acceptable plans, and subsequent optimization for final plans was completed by Monaco without further intervention. The plan quality was weakly dependent on the parameter selection in the initial template and the choices of the step sizes for changing the constraint values.
Conclusion: An automated planning platform to interface with Monaco was developed, and our reported tests showed preliminary results for prostate and head and neck cases.
Keywords: VMAT; auto-planning; inverse planning; template.
© 2020 The Authors. Journal of Applied Clinical Medical Physics published by Wiley Periodicals, Inc. on behalf of American Association of Physicists in Medicine.
Conflict of interest statement
No Conflicts of Interest.
Figures


References
-
- Yan H, Yin F, Guan H, et al. Fuzzy logic guided inverse treatment planning. Med Phys. 2003;30:2675–2685. - PubMed
-
- Yan H, Yin F, Guan H, et al. AI‐guided parameter optimization in inverse treatment planning. Phys Med Biol. 2003;48:3565. - PubMed
-
- Yan H, Yin F, Willett C. Evaluation of an artificial intelligence guided inverse planning system: clinical case study. Radiother Oncol. 2007;83:76–85. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
