

Comprehensive Evaluation of Relapse Risk (CERR) Score for Colorectal Liver Metastases: Development and Validation
- PMID: 32181531
- PMCID: PMC7356794
- DOI: 10.1634/theoncologist.2019-0797
Comprehensive Evaluation of Relapse Risk (CERR) Score for Colorectal Liver Metastases: Development and Validation
Abstract
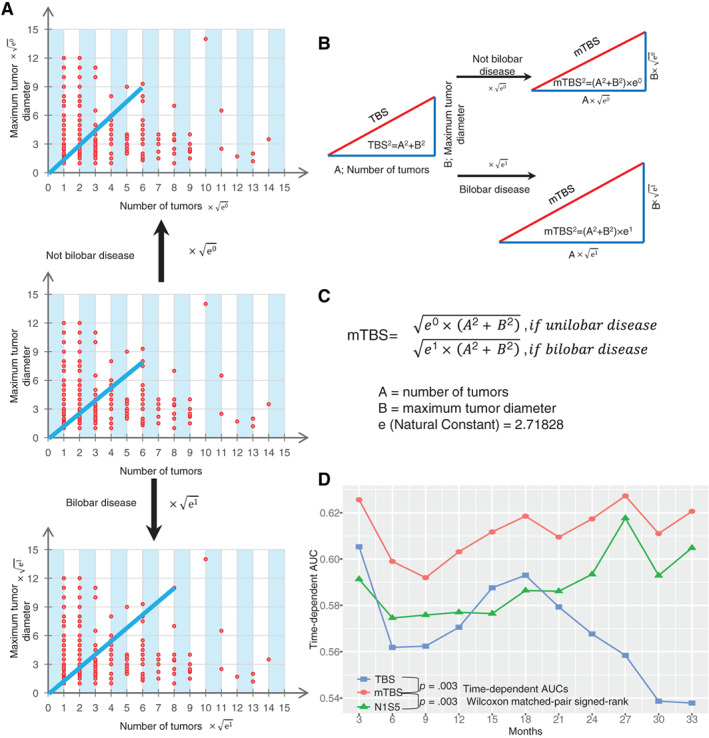
Background: The calculation of the tumor burden score (TBS) is not perfect because the bilobar spread of colorectal liver metastasis (CRLM) is neglected. The identification of an ideal prognostic scoring system for CRLM remains controversial.
Materials and methods: Patients who underwent curative intent liver resection for CRLM from one medical center were enrolled in cohort 1 (787 patients) and cohort 2 (162 patients). Tumor relapse-free survival (RFS) was the main outcome. A Cox regression model was used to identify independent predictors of prognosis. The time-dependent area under the curve, calibration curve, and C-index were employed to validate the predictive ability of the survival model.
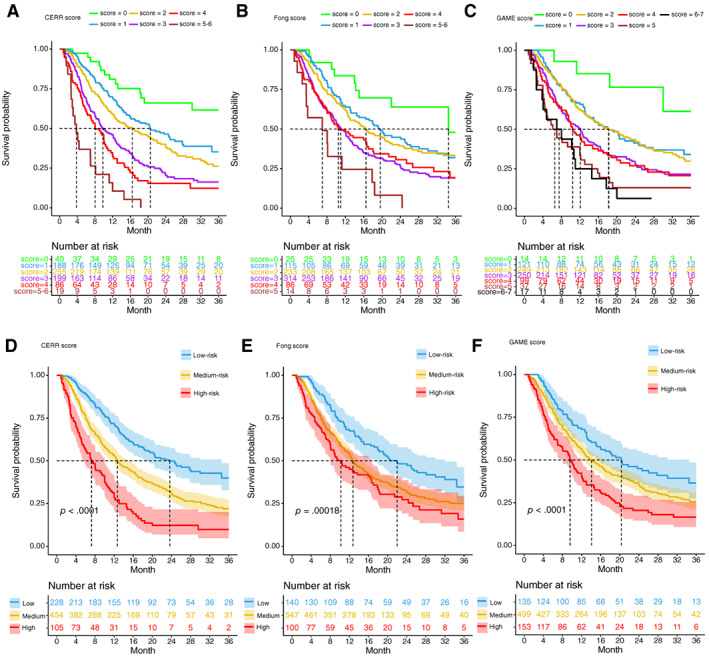
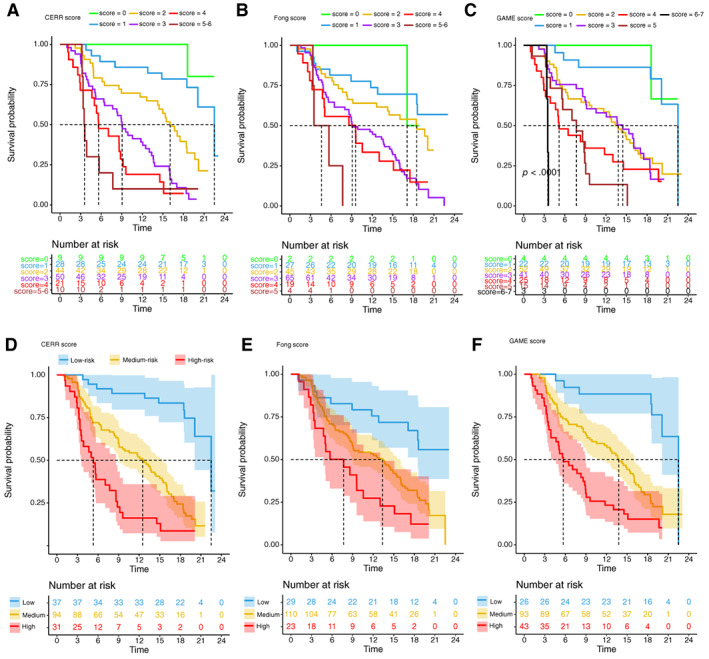
Results: Modified TBS (mTBS) was established by a mathematical equation with parameters including CRLM size, CRLM number, and unilobar or bilobar metastasis. Five preoperative predictors of worse RFS were identified in cohort 1 and incorporated into the Comprehensive Evaluation of Relapse Risk (CERR) score: KRAS/NRAS/BRAF-mutated tumor (1 point); node-positive primary (1 point); extrahepatic disease (1 point); carcinoembryonic antigen level > 200 ng/mL or carbohydrate antigen 19-9 (CA19-9) >200 U/mL (1 point); and mTBS between 5 and 11 (1 point) or 12 and over (2 points). Patients in cohort 1 were stratified by their CERR score into risk groups: the high-risk group (CERR score 4 or more), the medium-risk group (CERR score 2-3), and the low-risk group (CERR score 0-1). Importantly, internal validation in cohort 1 and further validation in cohort 2 both showed the superior discriminatory capacity of the CERR score.
Conclusion: mTBS should be promoted. The CERR score is a powerful prognostic tool that can help determine optimal clinical management strategies.
Implications for practice: This work resulted in the successful modification of the tumor burden score and development of a comprehensive and practical prognostic scoring system-the Comprehensive Evaluation of Relapse Risk (CERR) score. The CERR score, with a better prognostic discriminatory ability, outperformed the Fong score. Perhaps more importantly, the CERR score is a powerful prognostic tool because it unified the most consistently reported prognostic factors. Therefore, the CERR score can assist doctors in determining optimal clinical management strategies.
Keywords: Colorectal cancer; Hepatectomy; Metastasis; Prognosis; Relapse.
© AlphaMed Press 2020.
Conflict of interest statement
Figures

References
-
- Bray F, Ferlay J, Soerjomataram I et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018;68:394–424. - PubMed
-
- Van Cutsem E, Nordlinger B, Cervantes A; ESMO Guidelines Working Group. Advanced colorectal cancer: ESMO Clinical Practice Guidelines for treatment. Ann Oncol 2010;(Suppl 5):v93–v97. - PubMed
-
- de Jong MC, Pulitano C, Ribero D et al. Rates and patterns of recurrence following curative intent surgery for colorectal liver metastasis: An international multi‐institutional analysis of 1669 patients. Ann Surg 2009;250:440–448. - PubMed
-
- Nordlinger B, Guiguet M, Vaillant JC et al. Surgical resection of colorectal carcinoma metastases to the liver. A prognostic scoring system to improve case selection, based on 1568 patients. Association Francaise de Chirurgie. Cancer 1996;77:1254–1262. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
