

Efficacy and safety of anlotinib, a multikinase angiogenesis inhibitor, in combination with epirubicin in preclinical models of soft tissue sarcoma
- PMID: 32181596
- PMCID: PMC7221313
- DOI: 10.1002/cam4.2941
Efficacy and safety of anlotinib, a multikinase angiogenesis inhibitor, in combination with epirubicin in preclinical models of soft tissue sarcoma
Abstract
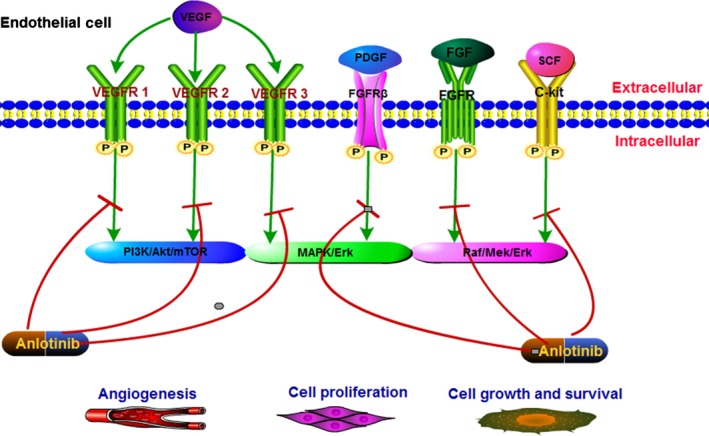
Background: Anlotinib is a novel, orally administered, multitarget receptor tyrosine kinase inhibitor. It functions by inhibiting tumor angiogenesis and proliferative signaling pathways. In this study, we aimed to investigate the efficacy and safety of anlotinib plus epirubicin in a sarcoma patient-derived xenografts (PDX) model.
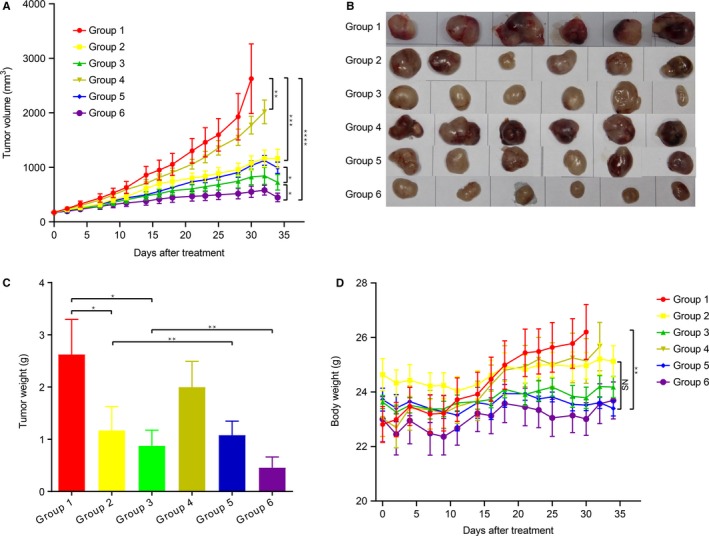
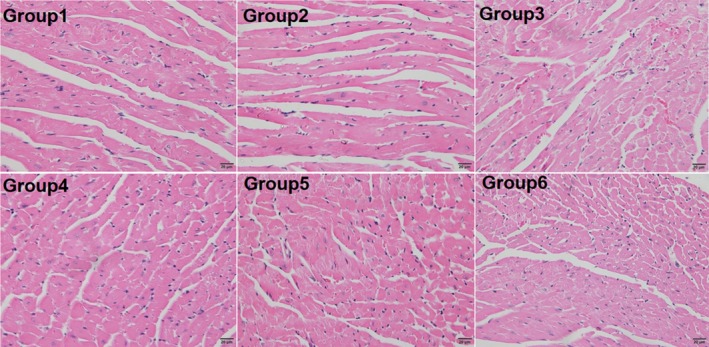
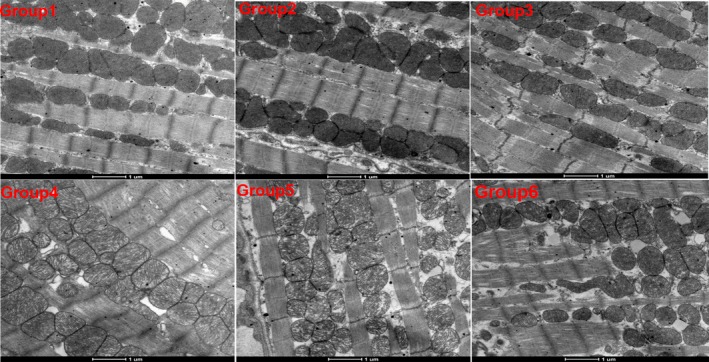
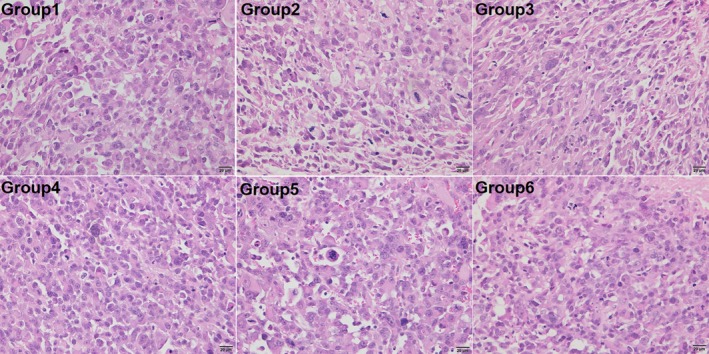
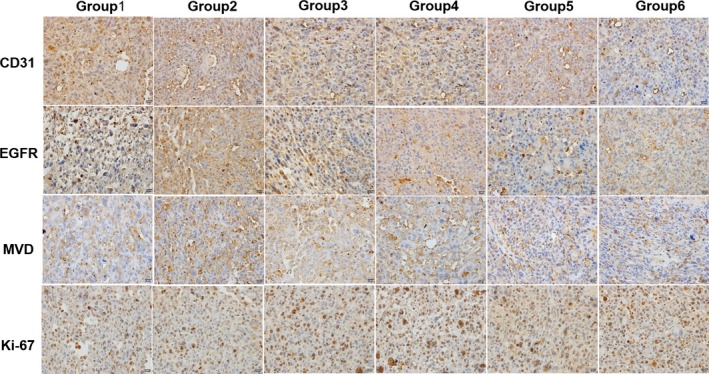
Methods: We firstly established a PDX model using fresh tumor tissues that were surgically removed from a patient diagnosed with malignant fibrous histiocytoma. Thirty-six PDX models were divided into six groups and treated with anlotinib alone (low-dose, 1.5 or high-dose, 3.0 mg/kg/day, oral gavage), or with anlotinib plus epirubicin (3.0 mg/kg/once weekly, i.p.) when the tumors grew to 150-200 mm3 . After 5 weeks of treatment, the mice were sacrificed, and the tumors were measured by weight and processed for IHC and H&E staining. IHC staining was performed to detect CD31, EGFR, MVD, and Ki-67 on paraffin sections. H&E stainings were performed to examine the microcosmic changes that occurred in the tumor tissues and myocardium, respectively.
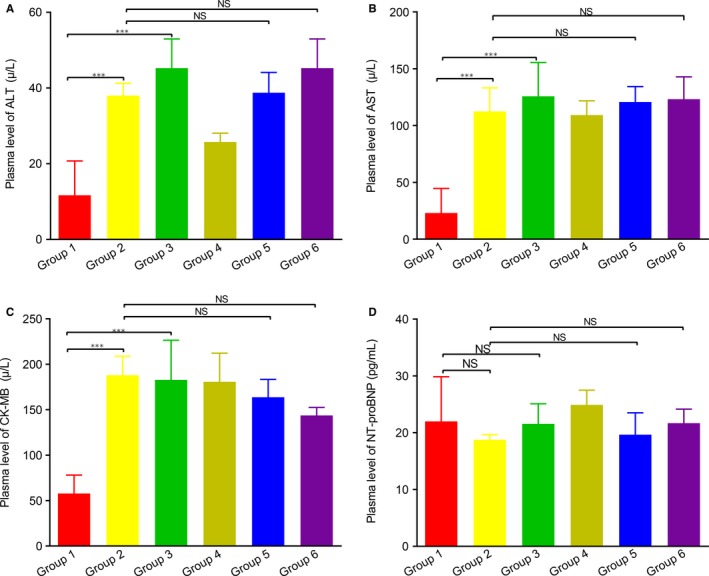
Results: After 5 weeks, treatment with anlotinib or epirubicin alone significantly inhibited tumor growth in the sarcoma PDX model compared with the vehicle control. Tumor volume in the high-dose anlotinib group was significantly smaller than the low-dose anlotinib group (P < .001). Combined high-dose anlotinib and epirubicin treatment resulted in the most pronounced tumor inhibition. In the groups treated with the anlotinib-containing regimen, the expression levels of CD31, EGFR, MVD, and Ki-67 were significantly low. The weight in each group had no statistical differences; the same applied to the hepatic function, cardiac function, and toxicity.
Conclusions: High-dose anlotinib combined with epirubicin was an effective and safe therapy for STS.
Keywords: anlotinib; combination; epirubicin; patient-derived xenografts; soft tissue sarcoma; tyrosine kinase inhibitor.
© 2020 The Authors. Cancer Medicine published by John Wiley & Sons Ltd.
Conflict of interest statement
All the authors have no conflicts of interested to declare.
Figures
References
-
- Cormier JN, Pollock RE. Soft tissue sarcomas. CA Cancer J Clin. 2004;54:94‐109. - PubMed
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin. 2018;60:277‐300. - PubMed
-
- Sbaraglia M, Dei AT. The pathology of soft tissue sarcomas. Radiol Med. 2019;124:266‐281. - PubMed
-
- Linch M, Miah AB, Thway K, Judson IR, Benson C. Systemic treatment of soft‐tissue sarcoma‐gold standard and novel therapies. Nat Rev Clin Oncol. 2014;11:187‐202. - PubMed
-
- Sheng JY, Movva S. Systemic therapy for advanced soft tissue sarcoma. Surg Clin North Am. 2016;96:1141‐1156. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
