

Safety, tolerability, and immunogenicity of influenza vaccination with a high-density microarray patch: Results from a randomized, controlled phase I clinical trial
- PMID: 32181756
- PMCID: PMC7077342
- DOI: 10.1371/journal.pmed.1003024
Safety, tolerability, and immunogenicity of influenza vaccination with a high-density microarray patch: Results from a randomized, controlled phase I clinical trial
Abstract
Background: The Vaxxas high-density microarray patch (HD-MAP) consists of a high density of microprojections coated with vaccine for delivery into the skin. Microarray patches (MAPs) offer the possibility of improved vaccine thermostability as well as the potential to be safer, more acceptable, easier to use, and more cost-effective for the administration of vaccines than injection by needle and syringe (N&S). Here, we report a phase I trial using the Vaxxas HD-MAP to deliver a monovalent influenza vaccine that was to the best of our knowledge the first clinical trial to evaluate the safety, tolerability, and immunogenicity of lower doses of influenza vaccine delivered by MAPs.
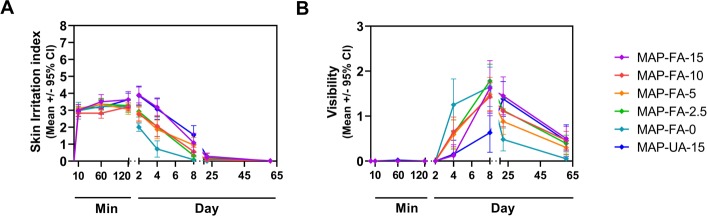
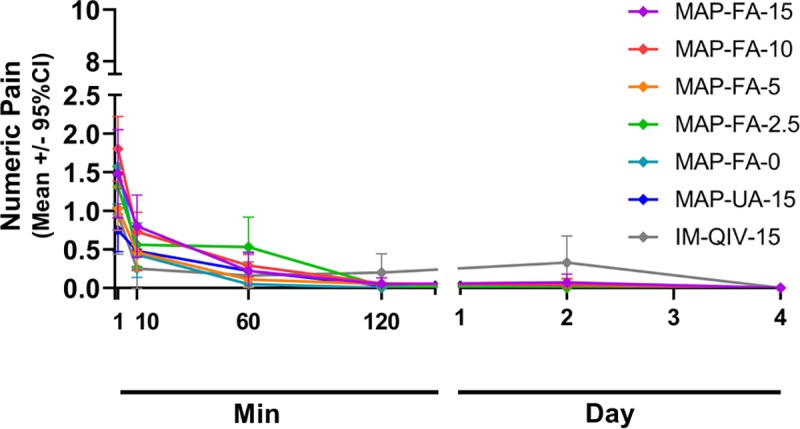
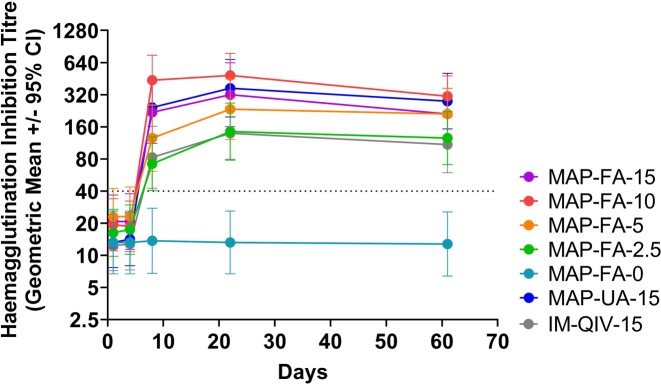
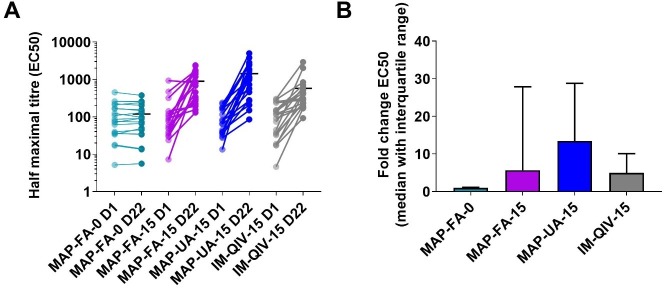
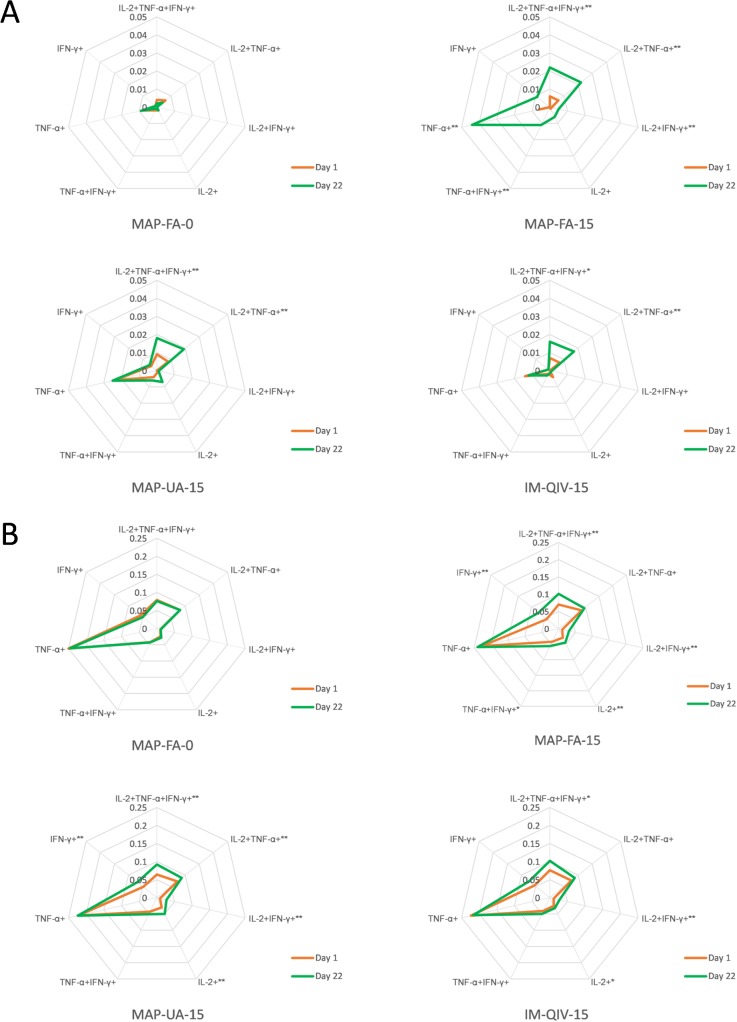
Methods and findings: HD-MAPs were coated with a monovalent, split inactivated influenza virus vaccine containing A/Singapore/GP1908/2015 H1N1 haemagglutinin (HA). Between February 2018 and March 2018, 60 healthy adults (age 18-35 years) in Melbourne, Australia were enrolled into part A of the study and vaccinated with either: HD-MAPs delivering 15 μg of A/Singapore/GP1908/2015 H1N1 HA antigen (A-Sing) to the volar forearm (FA); uncoated HD-MAPs; intramuscular (IM) injection of commercially available quadrivalent influenza vaccine (QIV) containing A/Singapore/GP1908/2015 H1N1 HA (15 μg/dose); or IM injection of H1N1 HA antigen (15 μg/dose). After 22 days' follow-up and assessment of the safety data, a further 150 healthy adults were enrolled and randomly assigned to 1 of 9 treatment groups. Participants (20 per group) were vaccinated with HD-MAPs delivering doses of 15, 10, 5, 2.5, or 0 μg of HA to the FA or 15 μg HA to the upper arm (UA), or IM injection of QIV. The primary objectives of the study were safety and tolerability. Secondary objectives were to assess the immunogenicity of the influenza vaccine delivered by HD-MAP. Primary and secondary objectives were assessed for up to 60 days post-vaccination. Clinical staff and participants were blind as to which HD-MAP treatment was administered and to administration of IM-QIV-15 or IM-A/Sing-15. All laboratory investigators were blind to treatment and participant allocation. Two further groups in part B (5 participants per group), not included in the main safety and immunological analysis, received HD-MAPs delivering 15 μg HA or uncoated HD-MAPs applied to the forearm. Biopsies were taken on days 1 and 4 for analysis of the cellular composition from the HD-MAP application sites. The vaccine coated onto HD-MAPs was antigenically stable when stored at 40°C for at least 12 months. HD-MAP vaccination was safe and well tolerated; any systemic or local adverse events (AEs) were mild or moderate. Observed systemic AEs were mostly headache or myalgia, and local AEs were application-site reactions, usually erythema. HD-MAP administration of 2.5 μg HA induced haemagglutination inhibition (HAI) and microneutralisation (MN) titres that were not significantly different to those induced by 15 μg HA injected IM (IM-QIV-15). HD-MAP delivery resulted in enhanced humoral responses compared with IM injection with higher HAI geometric mean titres (GMTs) at day 8 in the MAP-UA-15 (GMT 242.5, 95% CI 133.2-441.5), MAP-FA-15 (GMT 218.6, 95% CI 111.9-427.0), and MAP-FA-10 (GMT 437.1, 95% CI 254.3-751.3) groups compared with IM-QIV-15 (GMT 82.8, 95% CI 42.4-161.8), p = 0.02, p = 0.04, p < 0.001 for MAP-UA-15, MAP-FA-15, and MAP-FA-10, respectively. Higher titres were also observed at day 22 in the MAP-FA-10 (GMT 485.0, 95% CI 301.5-780.2, p = 0.001) and MAP-UA-15 (367.6, 95% CI 197.9-682.7, p = 0.02) groups compared with the IM-QIV-15 group (GMT 139.3, 95% CI 79.3-244.5). Results from a panel of exploratory immunoassays (antibody-dependent cellular cytotoxicity, CD4+ T-cell cytokine production, memory B cell (MBC) activation, and recognition of non-vaccine strains) indicated that, overall, Vaxxas HD-MAP delivery induced immune responses that were similar to, or higher than, those induced by IM injection of QIV. The small group sizes and use of a monovalent influenza vaccine were limitations of the study.
Conclusions: Influenza vaccine coated onto the HD-MAP was stable stored at temperatures up to 40°C. Vaccination using the HD-MAP was safe and well tolerated and resulted in immune responses that were similar to or significantly enhanced compared with IM injection. Using the HD-MAP, a 2.5 μg dose (1/6 of the standard dose) induced HAI and MN titres similar to those induced by 15 μg HA injected IM.
Trial registration: Australian New Zealand Clinical Trials Registry (ANZCTR.org.au), trial ID 108 ACTRN12618000112268/U1111-1207-3550.
Conflict of interest statement
I have read the journal's policy and the authors of this manuscript have the following competing interests: AHF, KW, ACID are paid employees of Vaxxas Pty Ltd. JWW, PT, GJPF and JH received consulting fees from Vaxxas Pty Ltd. JWW and MV are employees of the University of Queensland which carried out work for the study on a contract basis paid for by Vaxxas Pty Ltd. MP is an employee of 360Biolabs Pty Ltd which carried out work for the study on a contract basis paid for by Vaxxas Pty Ltd. JDL is an employee of Nucleus Network which carried out work for the study on a contract basis paid for by Vaxxas Pty Ltd. BF is an employee of Avance Clinical (formerly CPR Pharma Services) which carried out work for the study on a contract basis paid for by Vaxxas Pty Ltd. AW is an employee of Melbourne University which carried out work for the study on a contract basis paid for by Vaxxas Pty Ltd. AW has received travel expenses from Vaxxas Pty Ltd to attend data-review meetings.
Figures




References
-
- Fernando GJP, Hickling J, Jayashi Flores CM, Griffin P, Anderson CD, Skinner SR, et al. Safety, tolerability, acceptability and immunogenicity of an influenza vaccine delivered to human skin by a novel high-density microprojection array patch (NanopatchTM). Vaccine. 2018. 18;36(26):3779–88. 10.1016/j.vaccine.2018.05.053 - DOI - PubMed
-
- Poirier D, Renaud F, Dewar V, Strodiot L, Wauters F, Janimak J, et al. Hepatitis B surface antigen incorporated in dissolvable microneedle array patch is antigenic and thermostable. Biomaterials. 2017. November;145:256–65. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
