

Relationships between Neonatal Nutrition and Growth to 36 Weeks' Corrected Age in ELBW Babies-Secondary Cohort Analysis from the Provide Trial
- PMID: 32183057
- PMCID: PMC7146349
- DOI: 10.3390/nu12030760
Relationships between Neonatal Nutrition and Growth to 36 Weeks' Corrected Age in ELBW Babies-Secondary Cohort Analysis from the Provide Trial
Abstract
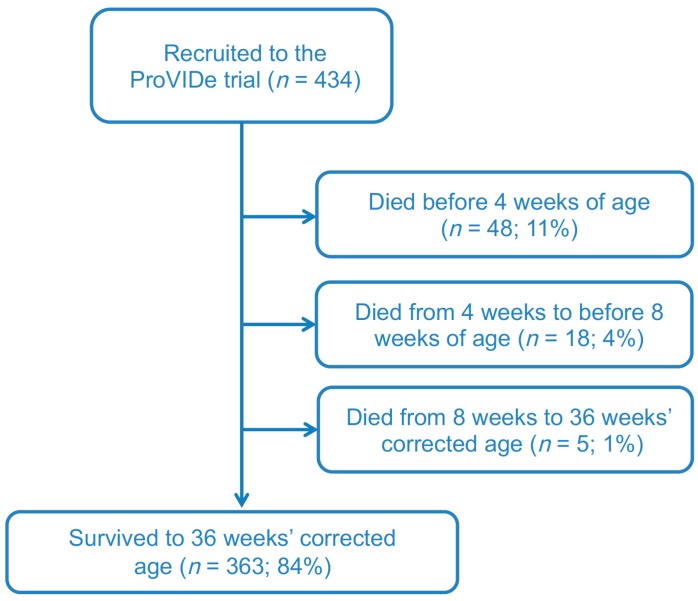
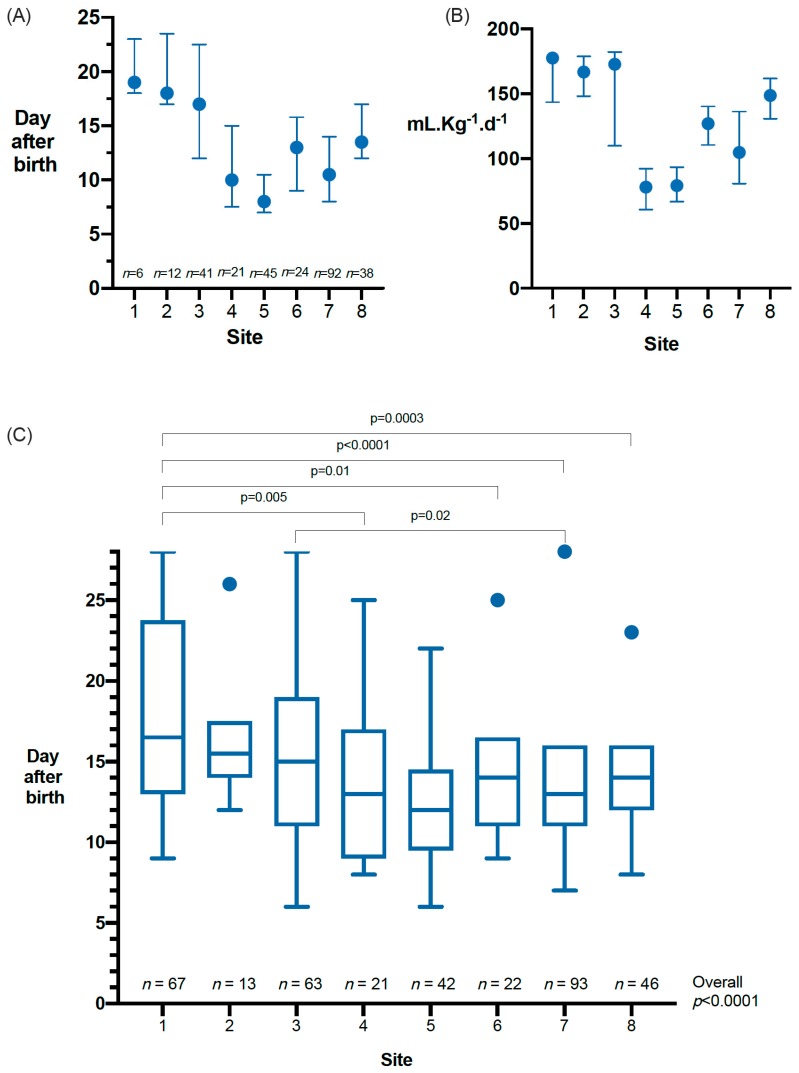
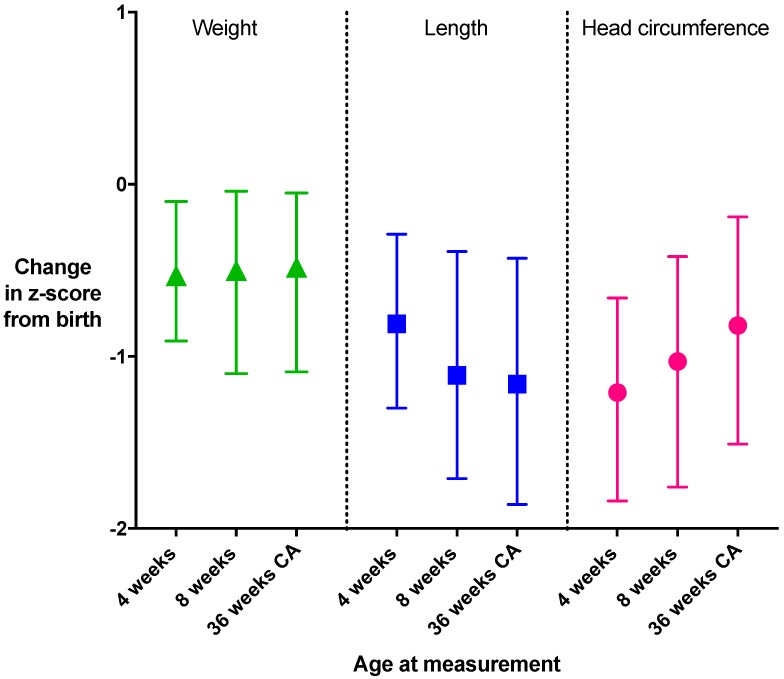
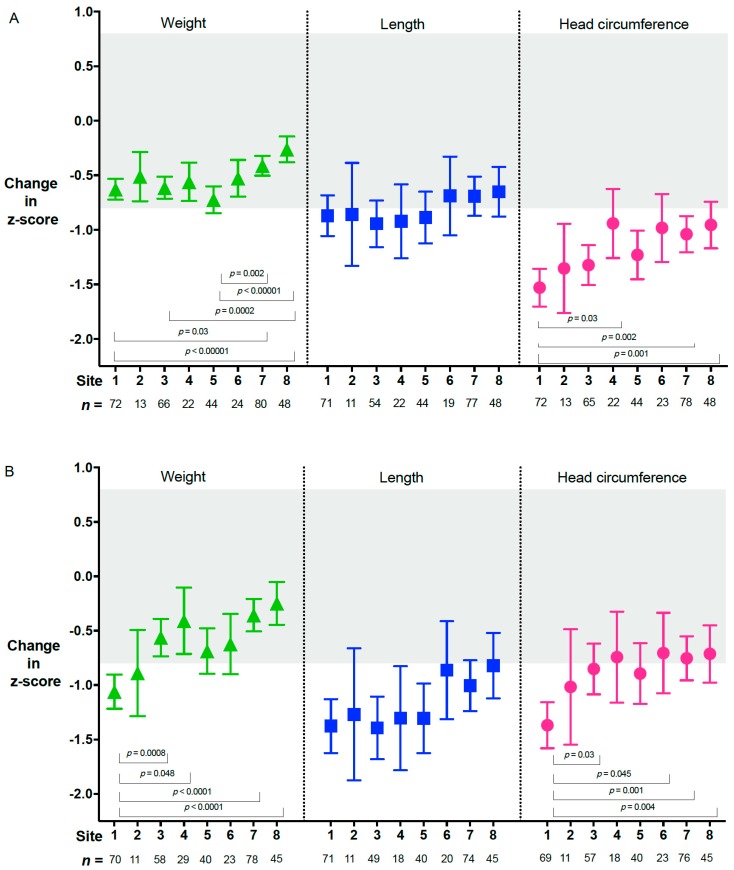
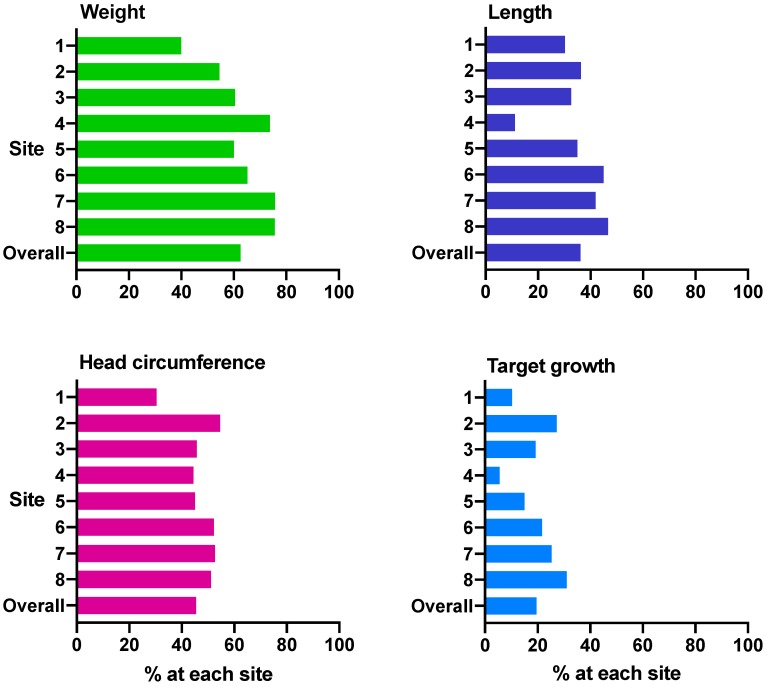
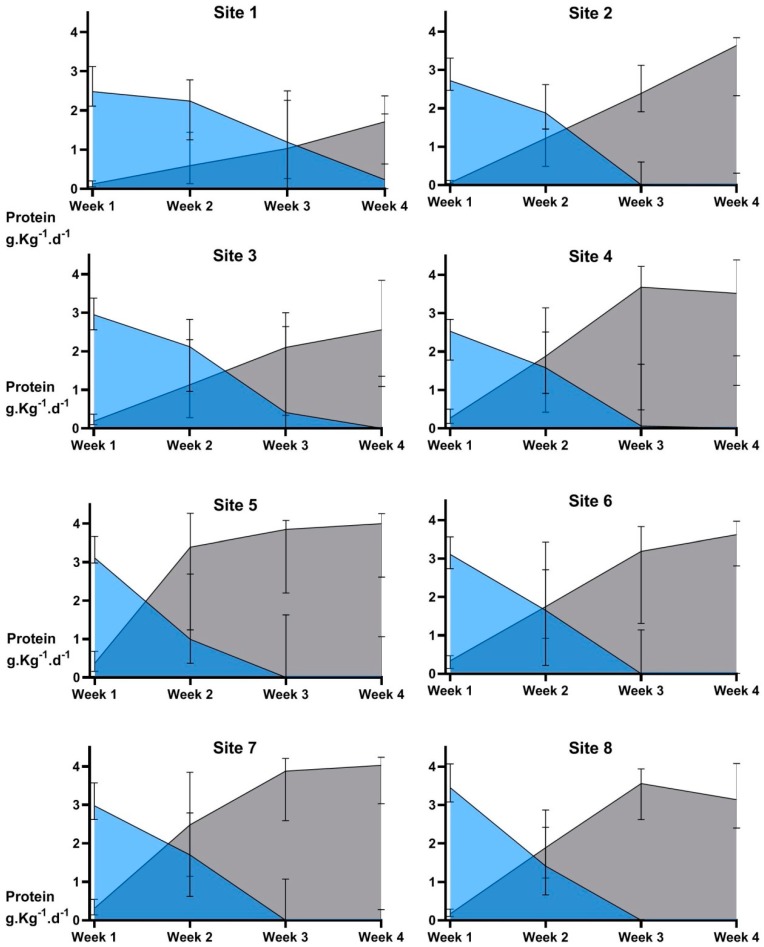
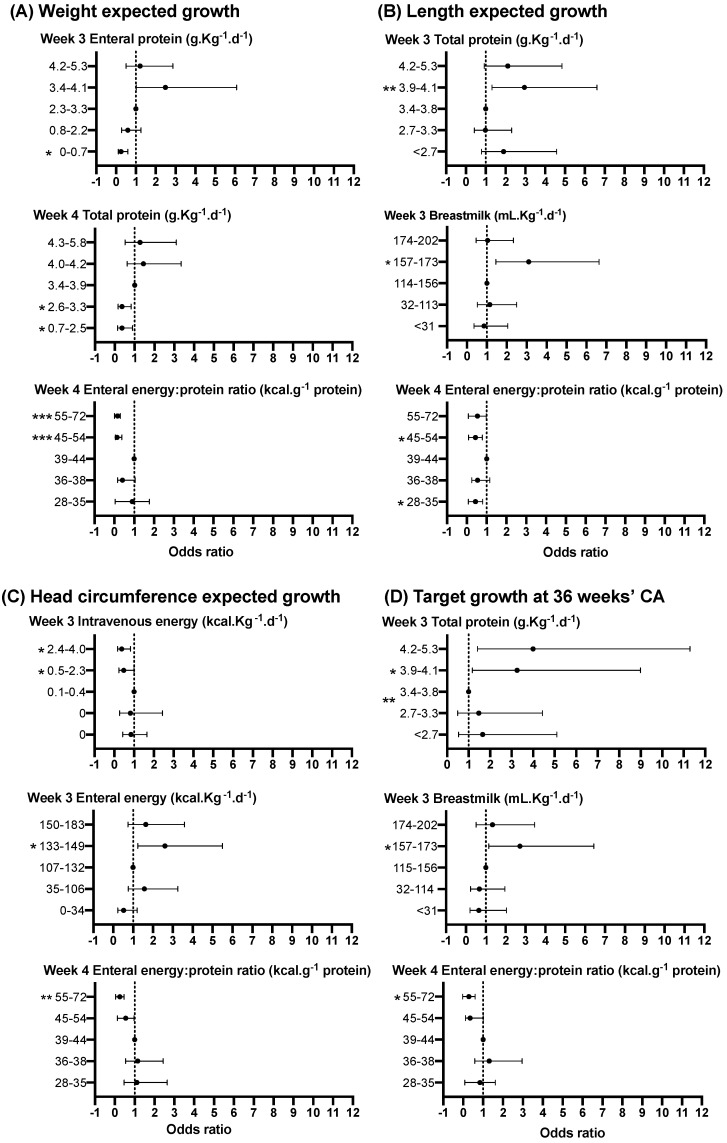
A key modifiable factor for improving neurodevelopment in extremely low birthweight (ELBW) babies may be improving growth, especially head growth, by optimising nutrition in the early neonatal period. We aimed to investigate relationships between nutrient intakes in the 4 weeks after birth, and growth from birth to 36 weeks' corrected age (CA) in ELBW babies. We undertook a prospective cohort study of 434 participants enrolled in a randomised controlled trial (ProVIDe) in eight New Zealand and Australian neonatal intensive care units. Macronutrient intakes from birth to 4 weeks and weight, length and head circumference measurements from birth to 36 weeks' CA were collected. From birth to 36 weeks' CA, the median (IQR) z-score changes were: weight -0.48 (-1.09, 0.05); length -1.16 (-1.86, -0.43), and head circumference -0.82 (-1.51, -0.19). Changes in z-score to 4 weeks and 36 weeks' CA were correlated with protein intake. Each 1 g·Kg-1·d-1 total protein intake in week 2 was associated with 0.26 z-score increase in head circumference at 36 weeks' CA. Both nutritional intake and change in z-scores to 36 weeks' CA differed widely amongst sites. Correlations between nutrition and growth, and differences in these amongst sites, indicate there may be potential to improve growth with enhanced nutrition practices.
Keywords: amino acid; extremely low birthweight; gestational age; growth; infant; newborn; nutrition; parenteral nutrition; premature; preterm; protein.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures
References
-
- Ziegler E.E., O’Donnell A.M., Nelson S.E., Fomon S.J. Body composition of the reference fetus. Growth. 1976;40:329–341. - PubMed
-
- Agostoni C., Buonocore G., Carnielli V.P., De Curtis M., Darmaun D., Decsi T., Domellof M., Embleton N.D., Fusch C., Genzel-Boroviczeny O., et al. Enteral nutrient supply for preterm infants: Commentary from the European Society of Paediatric Gastroenterology, Hepatology and Nutrition Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2010;50:85–91. doi: 10.1097/MPG.0b013e3181adaee0. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
