

Vitamin C Restricts the Emergence of Acquired Resistance to EGFR-Targeted Therapies in Colorectal Cancer
- PMID: 32183295
- PMCID: PMC7140052
- DOI: 10.3390/cancers12030685
Vitamin C Restricts the Emergence of Acquired Resistance to EGFR-Targeted Therapies in Colorectal Cancer
Abstract
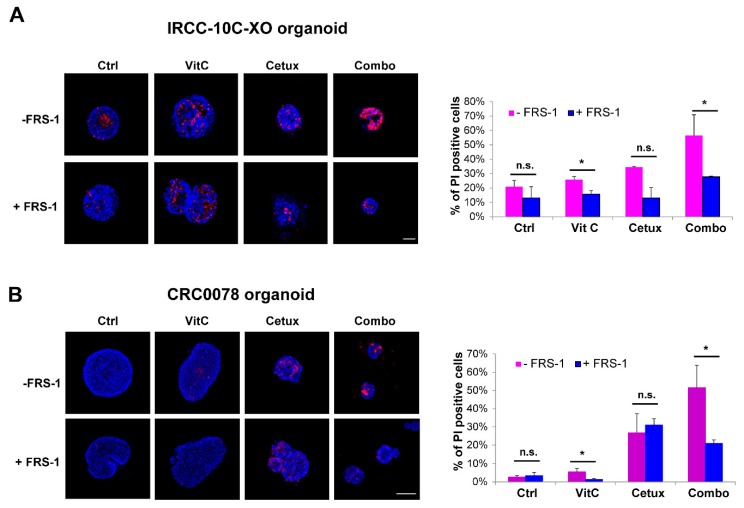
The long-term efficacy of the Epidermal Growth Factor Receptor (EGFR)-targeted antibody cetuximab in advanced colorectal cancer (CRC) patients is limited by the emergence of drug-resistant (persister) cells. Recent studies in other cancer types have shown that cells surviving initial treatment with targeted agents are often vulnerable to alterations in cell metabolism including oxidative stress. Vitamin C (VitC) is an antioxidant agent which can paradoxically trigger oxidative stress at pharmacological dose. Here we tested the hypothesis that VitC in combination with cetuximab could restrain the emergence of secondary resistance to EGFR blockade in CRC RAS/BRAF wild-type models. We found that addition of VitC to cetuximab impairs the emergence of drug persisters, limits the growth of CRC organoids, and significantly delays acquired resistance in CRC patient-derived xenografts. Mechanistically, proteomic and metabolic flux analysis shows that cetuximab blunts carbohydrate metabolism by blocking glucose uptake and glycolysis, beyond promoting slow but progressive ROS production. In parallel, VitC disrupts iron homeostasis and further increases ROS levels ultimately leading to ferroptosis. Combination of VitC and cetuximab orchestrates a synthetic lethal metabolic cell death program triggered by ATP depletion and oxidative stress, which effectively limits the emergence of acquired resistance to anti-EGFR antibodies. Considering that high-dose VitC is known to be safe in cancer patients, our findings might have clinical impact on CRC patients treated with anti-EGFR therapies.
Keywords: ROS; Vitamin C; cetuximab; colorectal cancer; drug resistance; ferroptosis; glucose metabolism; oxidative stress.
Conflict of interest statement
S. S. is an advisory board member for Amgen, Bayer, BMS, CheckmAb, Celgene, Daiichi-Sankyo, Incyte, Merck, Novartis, Roche, and Seattle Genetics; all the other authors declare no potential conflicts of interest.
Figures






Similar articles
-
Overcoming Intrinsic and Acquired Cetuximab Resistance in RAS Wild-Type Colorectal Cancer: An In Vitro Study on the Expression of HER Receptors and the Potential of Afatinib.Cancers (Basel). 2019 Jan 15;11(1):98. doi: 10.3390/cancers11010098. Cancers (Basel). 2019. PMID: 30650638 Free PMC article.
-
Blockade of EGFR and MEK intercepts heterogeneous mechanisms of acquired resistance to anti-EGFR therapies in colorectal cancer.Sci Transl Med. 2014 Feb 19;6(224):224ra26. doi: 10.1126/scitranslmed.3007947. Sci Transl Med. 2014. PMID: 24553387
-
MM-151 overcomes acquired resistance to cetuximab and panitumumab in colorectal cancers harboring EGFR extracellular domain mutations.Sci Transl Med. 2016 Feb 3;8(324):324ra14. doi: 10.1126/scitranslmed.aad5640. Sci Transl Med. 2016. PMID: 26843189 Clinical Trial.
-
Oncogenic fingerprint of epidermal growth factor receptor pathway and emerging epidermal growth factor receptor blockade resistance in colorectal cancer.World J Clin Oncol. 2016 Oct 10;7(5):340-351. doi: 10.5306/wjco.v7.i5.340. World J Clin Oncol. 2016. PMID: 27777877 Free PMC article. Review.
-
Resistance to anti-EGFR therapy in colorectal cancer: from heterogeneity to convergent evolution.Cancer Discov. 2014 Nov;4(11):1269-80. doi: 10.1158/2159-8290.CD-14-0462. Epub 2014 Oct 7. Cancer Discov. 2014. PMID: 25293556 Review.
Cited by
-
Unveiling ferroptosis as a promising therapeutic avenue for colorectal cancer and colitis treatment.Acta Pharm Sin B. 2024 Sep;14(9):3785-3801. doi: 10.1016/j.apsb.2024.05.025. Epub 2024 May 31. Acta Pharm Sin B. 2024. PMID: 39309484 Free PMC article. Review.
-
Ferroptosis in colorectal cancer: a future target?Br J Cancer. 2023 Apr;128(8):1439-1451. doi: 10.1038/s41416-023-02149-6. Epub 2023 Jan 26. Br J Cancer. 2023. PMID: 36703079 Free PMC article. Review.
-
Empowering Clinical Decision Making in Oligometastatic Colorectal Cancer: The Potential Role of Drug Screening of Patient-Derived Organoids.JCO Precis Oncol. 2021 Jul 21;5:PO.21.00143. doi: 10.1200/PO.21.00143. eCollection 2021 Jul. JCO Precis Oncol. 2021. PMID: 34327296 Free PMC article. No abstract available.
-
A ferroptosis associated gene signature for predicting prognosis and immune responses in patients with colorectal carcinoma.Front Genet. 2022 Sep 8;13:971364. doi: 10.3389/fgene.2022.971364. eCollection 2022. Front Genet. 2022. PMID: 36160009 Free PMC article.
-
Insights on Ferroptosis and Colorectal Cancer: Progress and Updates.Molecules. 2022 Dec 28;28(1):243. doi: 10.3390/molecules28010243. Molecules. 2022. PMID: 36615434 Free PMC article. Review.
References
-
- Misale S., Di Nicolantonio F., Sartore-Bianchi A., Siena S., Bardelli A. Resistance to anti-EGFR therapy in colorectal cancer: From heterogeneity to convergent evolution. Cancer Discov. 2014;4:1269–1280. doi: 10.1158/2159-8290.CD-14-0462. - DOI - PubMed
-
- Corcoran R.B., André T., Atreya C.E., Schellens J.H.M., Yoshino T., Bendell J.C., Hollebecque A., McRee A.J., Siena S., Middleton G., et al. Combined BRAF, EGFR, and MEK inhibition in patients with BRAFV600E-mutant colorectal cancer. Cancer Discov. 2018;8:428–443. doi: 10.1158/2159-8290.CD-17-1226. - DOI - PMC - PubMed
Grants and funding
- 20236/Associazione Italiana per la Ricerca sul Cancro
- 21091/Associazione Italiana per la Ricerca sul Cancro
- 635342-2 MoTriColor/Horizon 2020
- 21923/Associazione Italiana per la Ricerca sul Cancro
- Accelerator Award contract 22795/Associazione Italiana per la Ricerca sul Cancro
- TRANSCAN-2 JTC 2014 contract no. TRS-2015-00000060 INTRACOLOR/Horizon 2020
- TRANSCAN-2 JTC 2014 TACTIC/Horizon 2020
- 724748 - BEAT/ERC_/European Research Council/International
- 20697/Associazione Italiana per la Ricerca sul Cancro
- RC 2019/Ministero della Salute
- 5 per mille 2014 e 2015 Ministero della Salute/Fondazione Piemontese per la Ricerca sul Cancro-ONLUS
- 17707/Associazione Italiana per la Ricerca sul Cancro
- 20685/Associazione Italiana per la Ricerca sul Cancro
