

Acceptability and feasibility of testing for HIV infection at birth and linkage to care in rural and urban Zambia: a cross-sectional study
- PMID: 32183751
- PMCID: PMC7079396
- DOI: 10.1186/s12879-020-4947-6
Acceptability and feasibility of testing for HIV infection at birth and linkage to care in rural and urban Zambia: a cross-sectional study
Abstract
Background: Early infant diagnosis is important for timely identification of HIV-infected infants and linkage to care. Testing at birth has been implemented to facilitate earlier diagnosis of HIV infection but may present new challenges. This study was conducted to understand the acceptability and feasibility of birth testing in urban and rural settings in southern Zambia.
Methods: This cross-sectional study was conducted at 11 hospitals and clinics in Livingstone, Choma, and Macha in Southern Province, Zambia from 2016 to 2018. Infants born to pregnant women living with HIV at the sites were eligible for enrollment. After enrollment, a questionnaire was administered to the mother and a dried blood spot card was collected from infants for testing at a central laboratory. When results were available, mothers were notified to return to the clinic. Acceptability of birth testing was evaluated based on the proportion of women who agreed to participate and the reasons for non-participation among women who declined. Feasibility of testing at birth was evaluated using turnaround times for returning results, the proportion of women receiving results, and linkage to care for infants testing positive.
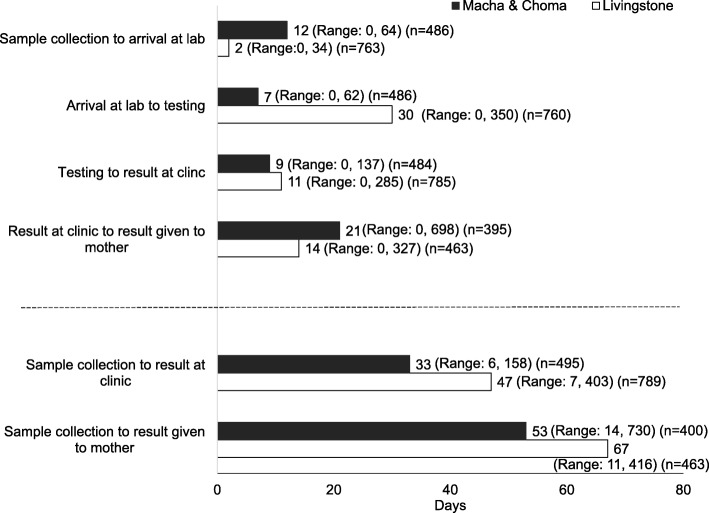
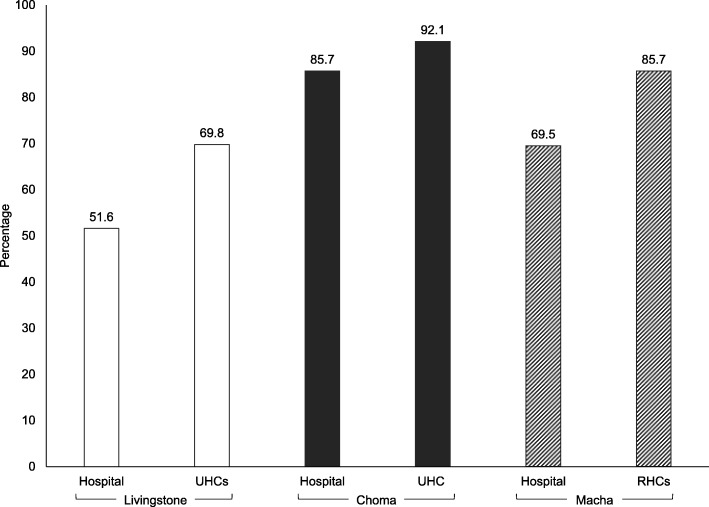
Results: One thousand four hundred three women were approached for the study. A small proportion declined due to refusal of birth testing (0 to 8.2% across sites). One thousand two hundred ninety women agreed to have their infants tested. The proportion of mothers receiving results ranged from 51.6 to 92.1%, and was significantly lower at the hospital than clinics in Livingstone (51.6% vs. 69.8%; p < 0.0001) and Macha (69.5% vs. 85.7%; p < 0.0001) but not Choma (85.7% vs. 92.1%; p = 0.34). For mothers who received test results, the median turnaround time from sample collection was 67 days in Livingstone and 53 days in Macha and Choma. Overall, 23 (1.8%) infants tested positive for HIV but only 8 (34.8%) were linked to care a median of 68 days (range: 29, 784) after sample collection.
Conclusions: While testing at birth was acceptable, this study highlights the operational challenges under a centralized laboratory testing system. Point-of-care platforms are needed for rapid testing and return of results so HIV-infected children can be identified, linked to care, and treated as early as possible.
Keywords: Early infant diagnosis; HIV; Linkage to care; Pediatrics; Sub-Saharan Africa; Zambia.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- WHO . WHO HIV update: global epidemic, progress in scale up and policy uptake. Geneva: World Health Organization; 2019.
-
- UNAIDS . 90–90-90: an ambitious treatment target to help end the AIDS epidemic. Geneva: Joint United Nations Programme on HIV/AIDS (UNAIDS); 2014.
-
- WHO . Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection. Recommendations for a public health approach. 2. Geneva: World Health Organization; 2016. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
