

Co-infections of human herpesviruses (CMV, HHV-6, HHV-7 and EBV) in non-transplant acute leukemia patients undergoing chemotherapy
- PMID: 32183884
- PMCID: PMC7079388
- DOI: 10.1186/s12985-020-01302-4
Co-infections of human herpesviruses (CMV, HHV-6, HHV-7 and EBV) in non-transplant acute leukemia patients undergoing chemotherapy
Abstract
Background: Human herpesviruses (HHVs) remain latent after primary infection and can be reactivated in response to immunosuppression and chemotherapy. Little is known about their incidence, potential relationships, risk factors and clinical impact in non-transplant leukemia patients. This study investigated prospectively incidence, risk factors, clinical impact and possible association of HHVs-(1-7) infections in patients with newly diagnosed acute leukemia.
Methods: Study design involved longitudinal sampling before chemotherapy and in different phases of chemotherapy: post-induction, post-remission, and post-salvage during 2016-2018. A total of 734 plasma samples from 95 patients were analyzed by a qualitative, multiplex PCR for HHVs detection and a quantitative real-time PCR was used for cytomegalovirus (CMV) quantification. HHVs-(1-6) IgG and IgM antibodies were tested using immunoassays. Risk factors were analyzed by binary logistic regression and relationships between viruses were analyzed using the Chi-square or Fisher's exact test as appropriate.
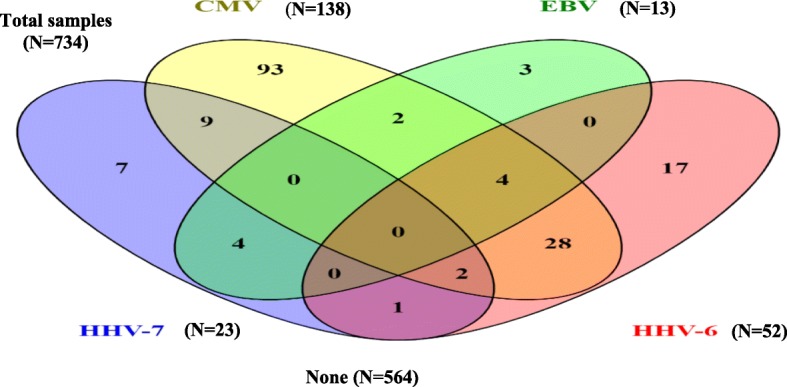
Results: The overall seroprevalences of HHV-(1-6) IgG were high (> 80%). At least one herpes viral agent was detected in 60 patients (63.3%). CMV was the most commonly detected virus in the different phases of chemotherapy (19.4%), followed by HHV-6 (9.7%), HHV-7 (5.2%) and EBV (2.7%). HSV-1/2 and VZV DNA were not detected. Twenty-seven patients (28.4%) had more than one virus detected in the follow-up, with 23 who were co-infected. CMV/HHV-6 was the most frequent co-infection (69.5%, 16/23). HHV-6 infection (p = 0.008) was identified as a risk factor for CMV infection while salvage treatment (p = 0.04) and CMV infection (p = 0.007) were found to be independent risk factors for HHV-6 infection. CMV co-infection was associated with severe lymphopenia with an absolute lymphocyte count (ALC) (< 500/μL) (p = 0.009), rash (p = 0.011), pneumonia (p = 0.016) and opportunistic infections [bacteremia, p < 0.001 and invasive fungal infection, (p = 0.024)] more frequently than CMV mono-viral infections.
Conclusions: Our data suggest that co-infection with HHVs, especially CMV and HHV-6, may contribute to the development of serious clinical manifestations with profound lymphopenia, pneumonia rash and increased risk for bacterial and fungal co-infections. These findings may suggest the synergistic effect of HHVs associated infection.
Keywords: Acute leukemia; Chemotherapy; Co-infection; Herpesviruses.
Conflict of interest statement
The authors declare that they have no competing.
Figures

References
-
- Rahbarimanesh A, Ehsani M, Karahroudi M, Rashidi A, Aghajani M, Meysami A, Shahgholi E, Mehrvar A, Tashvighi M, Keyvani H. Cytomegalovirus Disease in Children With Acute Lymphoblastic Leukemia in the Nontransplant Setting: Case Series and Review of the Literature. J Pediatr Hematol Oncol. 2015;37:429–432. doi: 10.1097/MPH.0000000000000298. - DOI - PubMed
-
- Torres HA, Aguilera E, Safdar A, Rohatgi N, Raad SC, II, Luna M, Kontoyiannis DP, Chemaly RF. Fatal cytomegalovirus pneumonia in patients with haematological malignancies: an autopsy-based case-control study. Clin Microbiol Infect. 2008;14:1160–1166. doi: 10.1111/j.1469-0691.2008.02106.x. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
