

Nephrology Fellows' and Program Directors' Perceptions of Hospital Rounds in the United States
- PMID: 32184295
- PMCID: PMC7133138
- DOI: 10.2215/CJN.10190819
Nephrology Fellows' and Program Directors' Perceptions of Hospital Rounds in the United States
Abstract
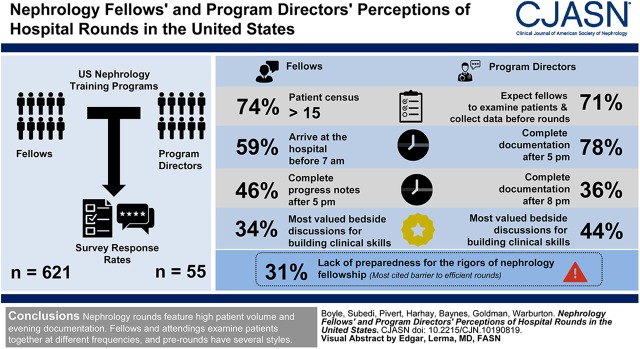
Background and objectives: Hospital rounds are a traditional vehicle for patient-care delivery and experiential learning for trainees. We aimed to characterize practices and perceptions of rounds in United States nephrology training programs.
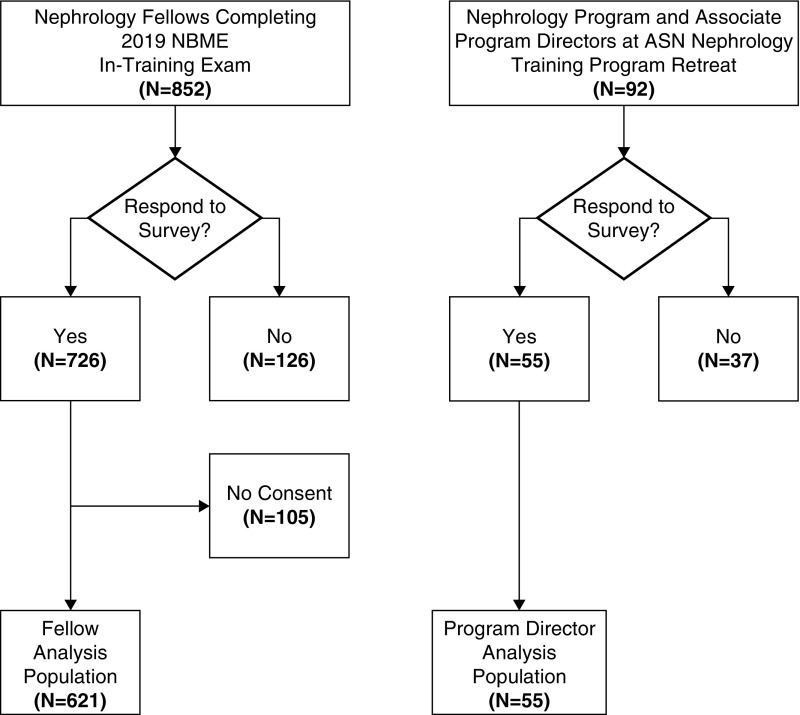
Design, setting, participants, & measurements: We conducted a national survey of United States nephrology fellows and program directors. Fellows received the survey after completing the 2019 National Board of Medical Examiners Nephrology In-Training Exam. Program directors received the survey at the American Society of Nephrology's 2019 Nephrology Training Program Directors' Retreat. Surveys assessed the structure and perceptions of rounds, focusing on workload, workflow, value for patient care, and fellows' clinical skill-building. Directors were queried about their expectations for fellow prerounds and efficiency of rounds. Responses were quantified by proportions.
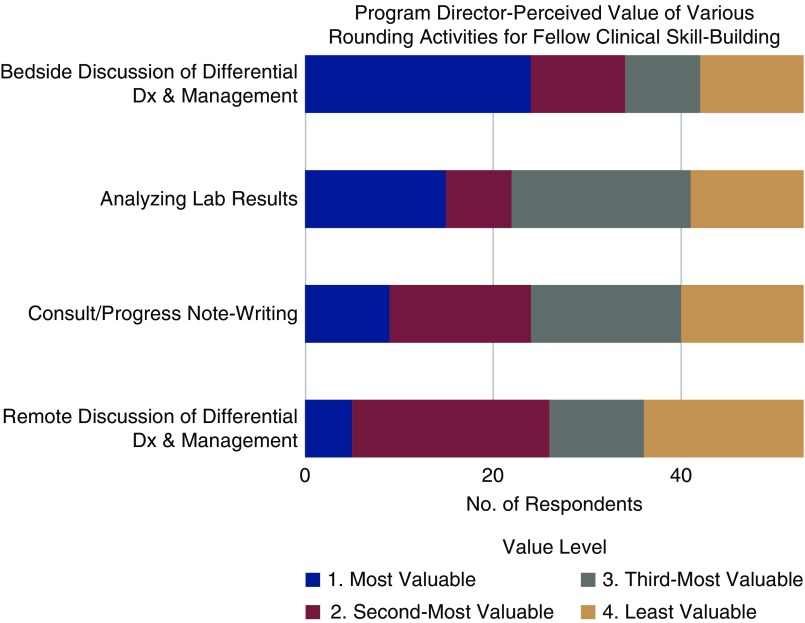
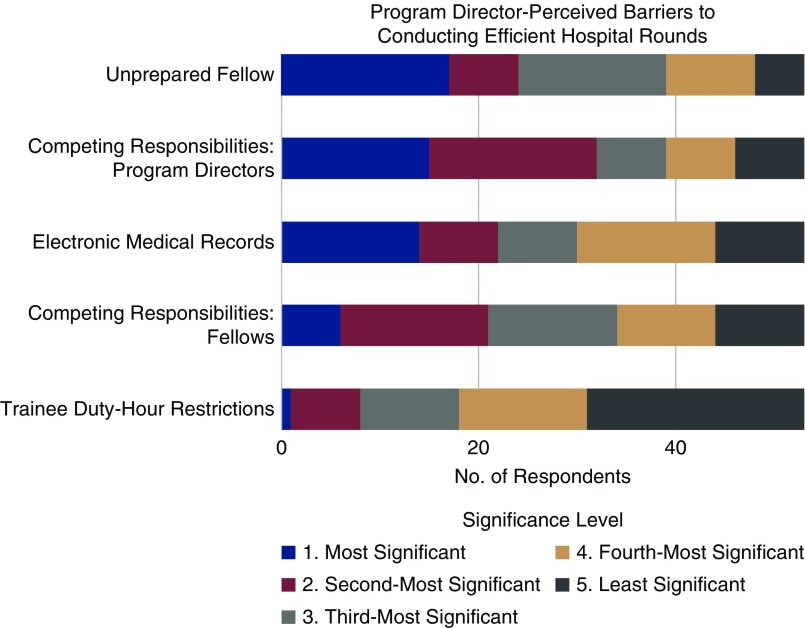
Results: Fellow and program director response rates were 73% (n=621) and 70% (n=55). Most fellows (74%) report a patient census of >15, arrive at the hospital before 7:00 am (59%), and complete progress notes after 5:00 pm (46%). Among several rounding activities, fellows most valued bedside discussions for building their clinical skills (34%), but only 30% examine all patients with the attending at the bedside. Most directors (71%) expect fellows to both examine patients and collect data before attending-rounds. A majority (78%) of directors commonly complete their documentation after 5:00 pm, and for 36%, after 8:00 pm. Like fellows, directors most value bedside discussion for development of fellows' clinical skills (44%). Lack of preparedness for the rigors of nephrology fellowship was the most-cited barrier to efficient rounds (31%).
Conclusions: Hospital rounds in United States nephrology training programs are characterized by high patient volumes, early-morning starts, and late-evening clinical documentation. Fellows use a variety of prerounding styles and examine patients at the beside with their attendings at different frequencies.
Podcast: This article contains a podcast at https://www.asn-online.org/media/podcast/CJASN/2020_03_17_CJN.10190819.mp3.
Keywords: Censuses; Clinical Competence; Documentation; Motivation; Patient Care; Problem-Based Learning; Records; Surveys and Questionnaires; Teaching Rounds; Training Support; Workflow; Workload; clinical nephrology.
Copyright © 2020 by the American Society of Nephrology.
Figures
References
-
- Accreditation Council for Graduate Medical Education ACGME Common Program Requirements (Fellowship), 2018. Available at: https://www.acgme.org/Portals/0/PFAssets/ProgramRequirements/CPRFellowsh.... Accessed July 15, 2019
-
- Wenger N, Méan M, Castioni J, Marques-Vidal P, Waeber G, Garnier A: Allocation of internal medicine resident time in a swiss hospital: A time and motion study of day and evening shifts. Ann Intern Med 166: 579–586, 2017 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
