

Microscope Integrated Intraoperative Optical Coherence Tomography-Guided DMEK in Corneas with Poor Visualization
- PMID: 32184553
- PMCID: PMC7060773
- DOI: 10.2147/OPTH.S230195
Microscope Integrated Intraoperative Optical Coherence Tomography-Guided DMEK in Corneas with Poor Visualization
Abstract
Purpose: To assess the utility of microscope-integrated intraoperative optical coherence tomography (Mi-OCT) for performing Descemet membrane endothelial keratoplasty (DMEK) in corneas with poor visualization.
Methods: It is a prospective interventional case series that included 25 consecutive cases of corneal decompensation with poor visualization that underwent Mi-OCT-guided DMEK at a tertiary eye care centre. The main outcome measures were graft attachment on day 3 and requirement for re-bubbling.
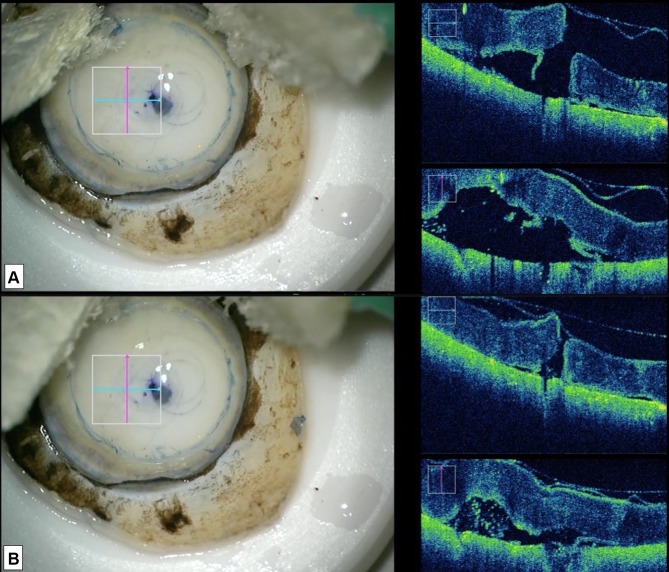
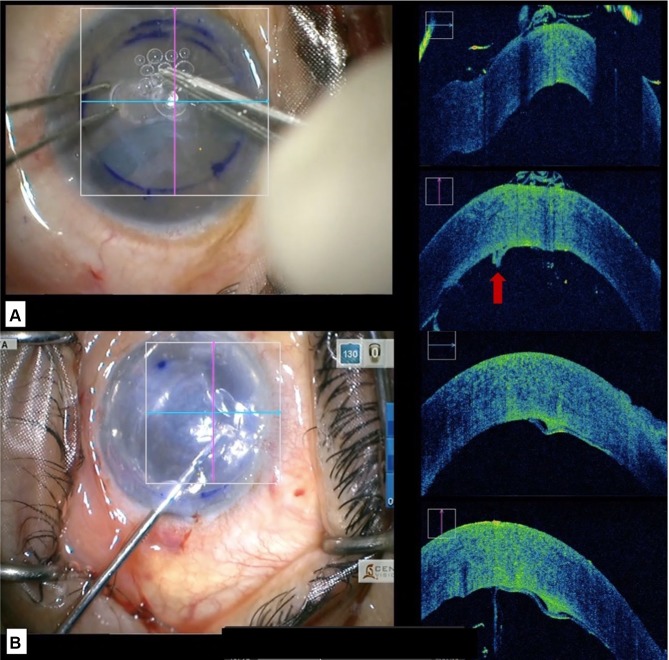
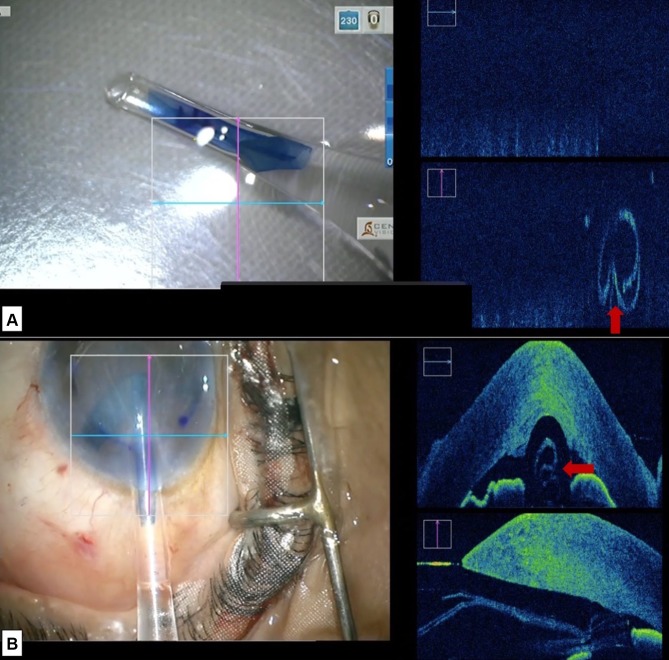
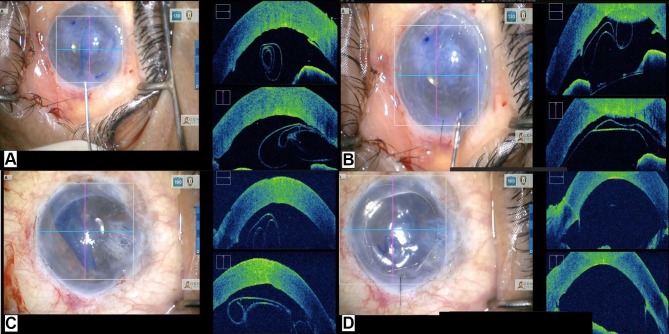
Results: The etiology for corneal decompensation was pseudophakic bullous keratopathy (n=17), Fuchs endothelial corneal dystrophy (n=4), failed graft (n=2), iridocorneal endothelial syndrome (n=1) and failed Descemet stripping automated endothelial keratoplasty (n=1). Complete graft attachment was noted in 72% of cases. Graft detachment was noted in 16% of cases which required re-bubbling. No intervention was done for shallow peripheral detachment (n=2) and peripheral Descemet membrane (DM) fold (n=1). All grafts were attached at six-months follow-up. The mean corrected distance visual acuity and central corneal thickness improved from 1.4 ± 0.5 logMAR and 799.6 ± 110.9 µm at baseline to 0.3 ± 0.3 logMAR and 536.28 ± 11.44 um at six months. Mi-OCT was helpful in visualizing areas of peripheral anterior synechiae, missing DM, retained DM tags after descemetorhexis, DMEK roll configuration and orientation in the injector and anterior chamber, interface fluid and peripheral folds in the DMEK graft.
Conclusion: Mi-OCT helps in identification of the anatomy and dynamics of the host DM, DM roll and anterior chamber in cases with poor visualization and is a useful tool while performing DMEK in such cases.
Keywords: DMEK; Mi-OCT; descemet membrane endothelial keratoplasty; iOCT; microscope-integrated intra-operative optical coherence tomography.
© 2020 Sharma et al.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures


References
-
- Singh A, Zarei-Ghanavati M, Avadhanam V, Liu C. Systematic review and meta-analysis of clinical outcomes of descemet membrane endothelial keratoplasty versus descemet stripping endothelial kerato - PubMed - NCBI. Available from: https://www.ncbi.nlm.nih.gov/pubmed/28834814. Accessed July23, 2018. - PubMed
LinkOut - more resources
Full Text Sources
