

A Population-Based Propensity Score-Matched Study to Assess the Impact of Repeated Vaccination on Vaccine Effectiveness for Influenza-Associated Hospitalization Among the Elderly
- PMID: 32184579
- PMCID: PMC7060795
- DOI: 10.2147/CIA.S238786
A Population-Based Propensity Score-Matched Study to Assess the Impact of Repeated Vaccination on Vaccine Effectiveness for Influenza-Associated Hospitalization Among the Elderly
Abstract
Background: Influenza is a major cause of morbidity and mortality in the elderly worldwide. Influenza vaccination can prevent morbidity/mortality from influenza infection. A gap of 1-2 years, before an epidemic strain is recommended by the World Health Organization (WHO) to be the vaccine strain in Southeast Asia, has been reported; this results in a high rate of vaccine mismatch and excess influenza-associated morbidity. The aim of the current study was to evaluate the effect of repeated vaccination on vaccine effectiveness (VE) among the elderly in Taiwan, during years with and without early appearance of antigenically drifted strains.
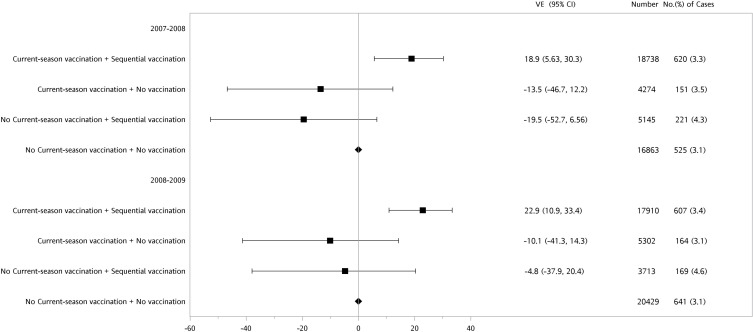
Methods: A historical cohort study was conducted to evaluate the impact of repeated vaccination on the reduction of influenza-associated hospitalization among persons older than 64 years over two influenza seasons: 2007-08, with all circulating virus strains mismatched, and 2008-09, with all virus strains matched with the vaccine strains, considering four exposure effects, namely current vaccine effect, sequential vaccination effect, residual protection effect and no vaccination effect. Propensity score matching on vaccination status was performed to ensure similar baseline characteristics between the groups that received and did not receive vaccination.
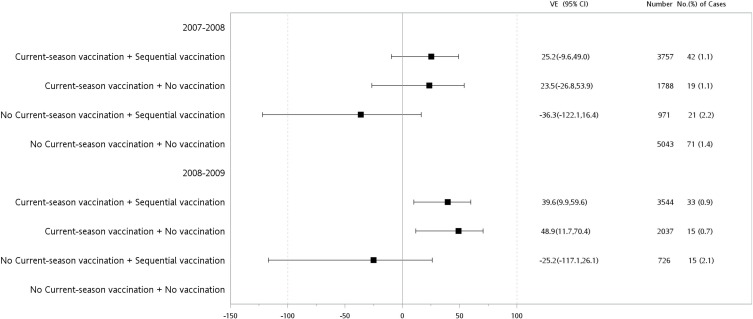
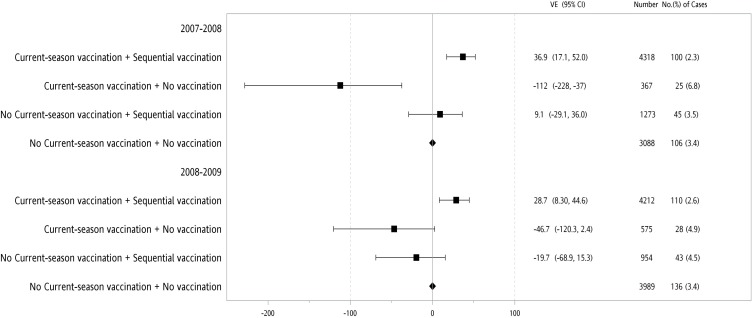
Results: Only current-year vaccination in combination with prior history of annual revaccination significantly reduced the risk of hospitalization, with adjusted hazard ratios of 0.68 (95% CI: 0.54, 0.85) and 0.74 (95% CI: 0.57, 0.95) during the 2007-08 and 2008-09 influenza seasons, respectively. Further stratification showed that even during the 2007-08 influenza season, when all vaccinations were mismatched with the circulating strains, sequential vaccinations still significantly reduced influenza-associated hospitalization in the female population aged 68-74 and 75-84 years, with adjusted VE of 25.2% (95% CI: -9.6, 49.0%) and 36.9% (95% CI: 17.1, 52.0%), respectively.
Conclusion: Our study supports the recommendation of annual revaccination against influenza in the elderly, even though the circulating strain of influenza virus was antigenically mismatched with the vaccine strains.
Keywords: elderly; prior vaccination history; propensity score matching; repeated vaccination; trivalent influenza vaccine; vaccine effectiveness.
© 2020 Hsu et al.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
