

Characteristics of Chronic Obstructive Pulmonary Disease Patients with Pulmonary Hypertension Assessed by Echocardiography in a Three-Year Observational Cohort Study
- PMID: 32184586
- PMCID: PMC7060780
- DOI: 10.2147/COPD.S230952
Characteristics of Chronic Obstructive Pulmonary Disease Patients with Pulmonary Hypertension Assessed by Echocardiography in a Three-Year Observational Cohort Study
Abstract
Background: Pulmonary hypertension (PH) is a major comorbidity of chronic obstructive pulmonary disease (COPD). However, the association of PH detected by echocardiography and COPD-related outcome in longitudinal follow-up has not been elucidated. In this study, we aimed to investigate the relationship between clinical characteristics of COPD patients with PH detected by echocardiography and various outcome parameters such as COPD exacerbation and health status over a three-year observation period.
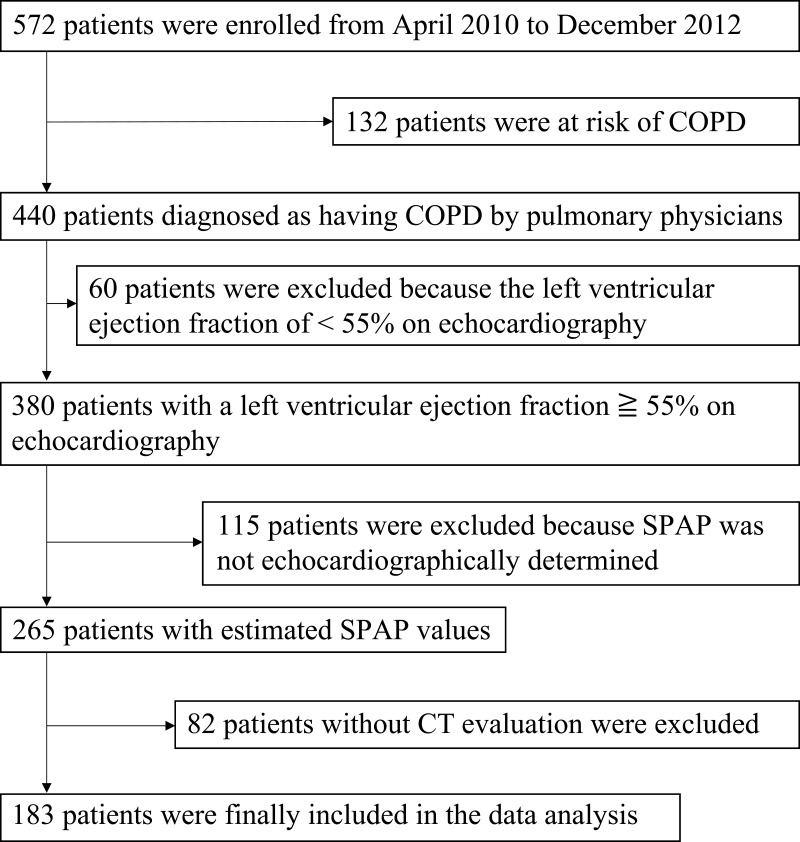
Methods: In this observational study, we analyzed patients with COPD who underwent chest computed tomography and echocardiography at baseline (n = 183).
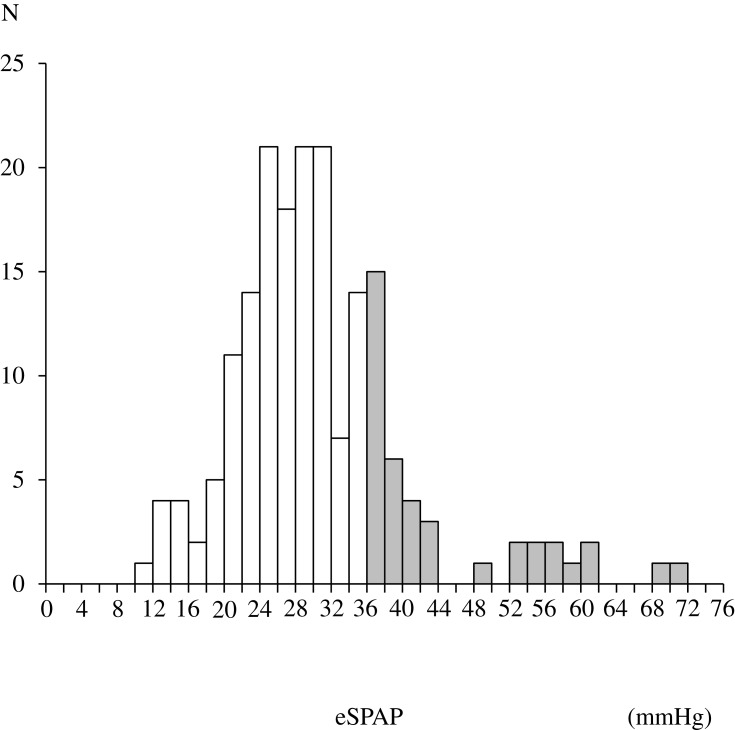
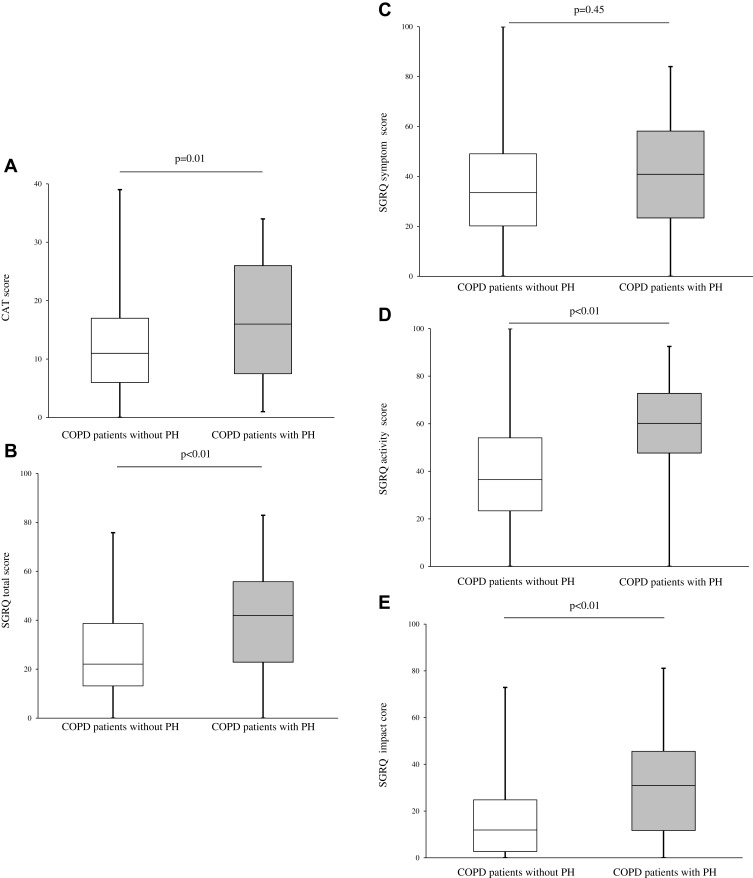
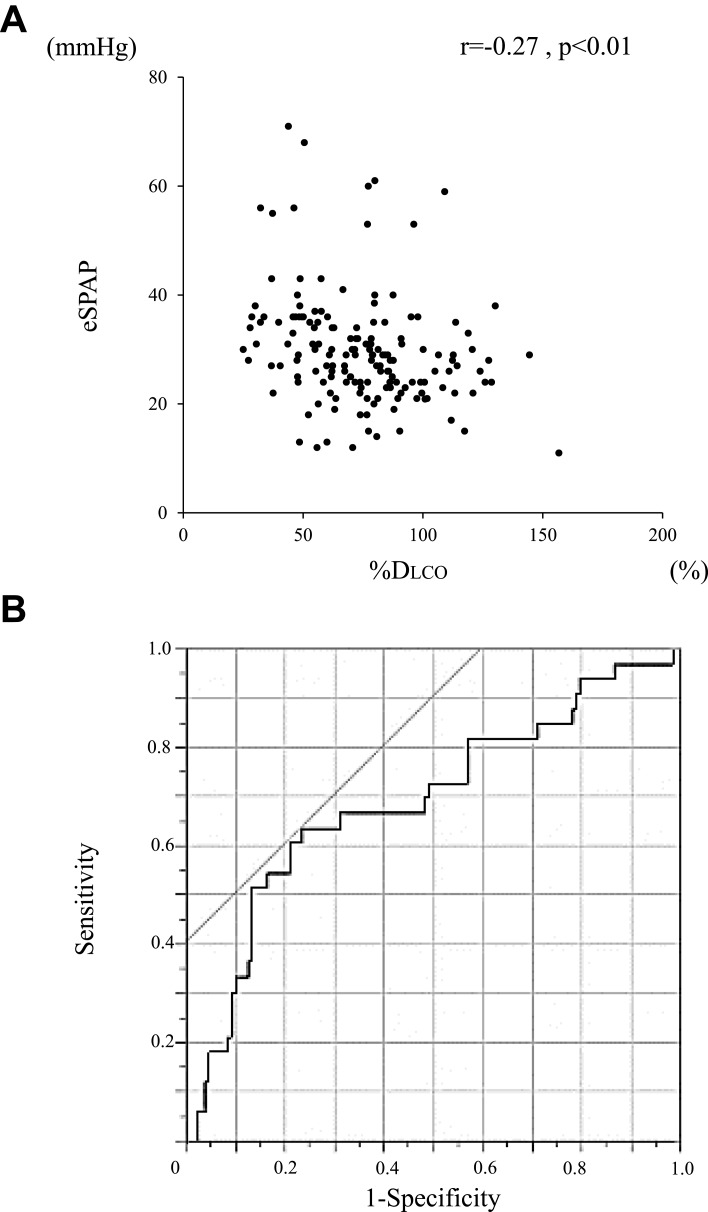
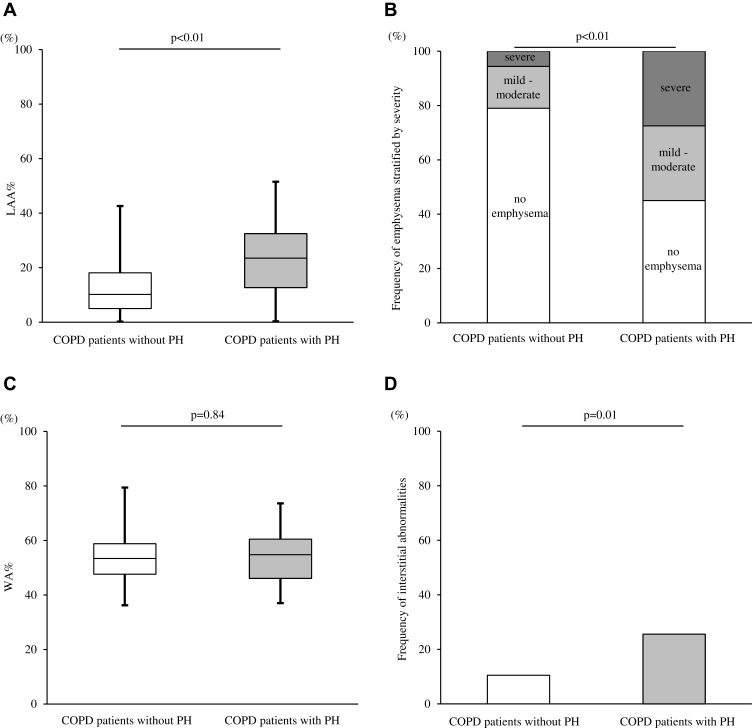
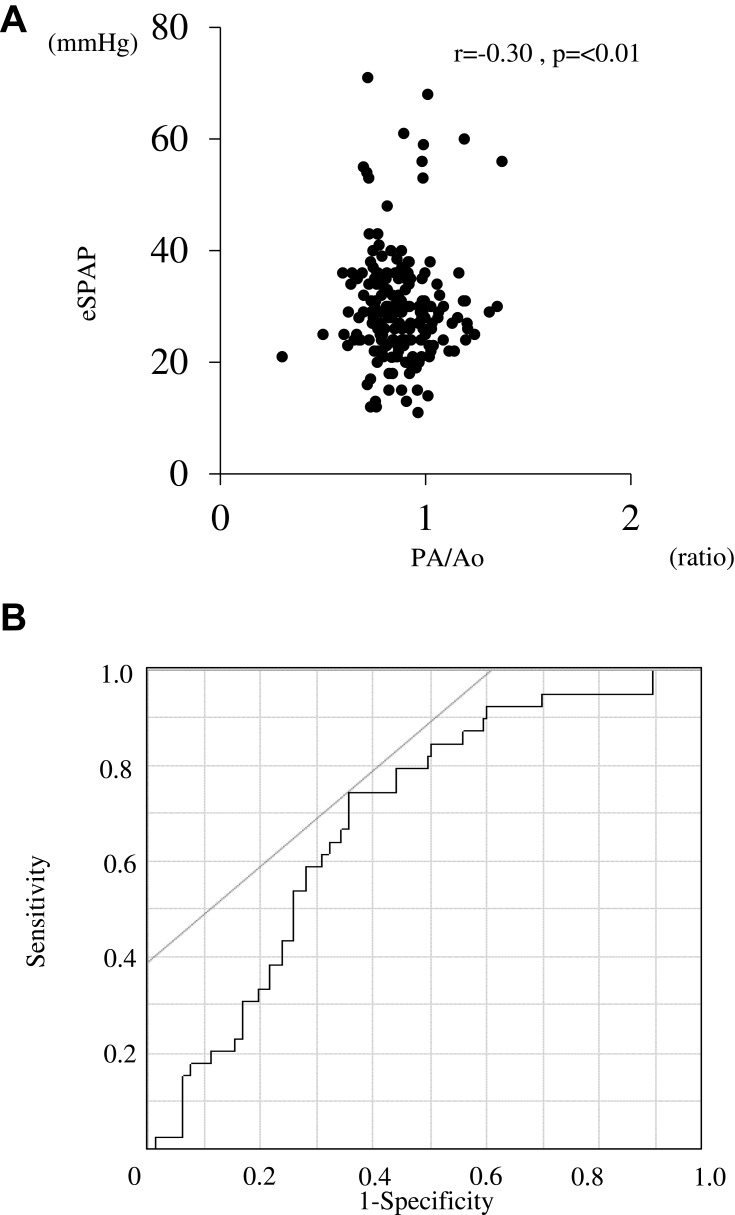
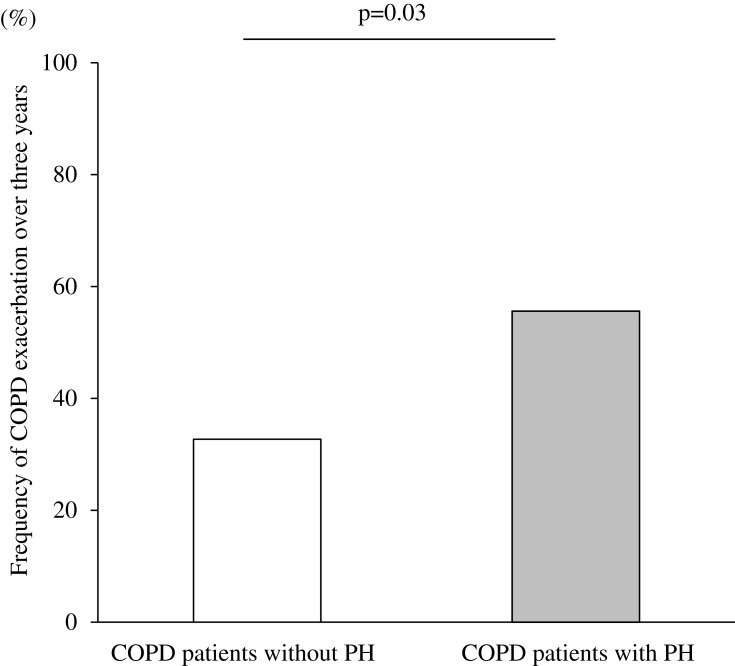
Results: The prevalence of PH was 21.9% (40 patients). The median estimated systolic pulmonary artery pressure in patients with PH was 38.8 mmHg. COPD patients with PH were older, had a lower body mass index, scored worse in the COPD Assessment Test and St. George's Respiratory Questionnaire, and exhibited a lower diffusing capacity of the lung for carbon monoxide in comparison to patients without PH. In computed tomography images, the percentages of low-attenuation areas (LAA%) and interstitial abnormalities were higher in COPD patients with PH than in those without PH. Higher values for LAA% (LAA ≥ 30%) and interstitial abnormalities independently increased the risk of PH. The ratio of main pulmonary diameter to aortic artery diameter was significantly correlated with estimated systolic pulmonary artery pressure. In the follow-up analysis, the frequency of exacerbations in three years was significantly higher in patients with PH compared to patients without PH.
Conclusion: In this study, we identified the clinical characteristics of COPD patients with PH detected by echocardiography. The presence of PH assessed by echocardiography was related to future COPD exacerbations and closely related to radiographical emphysema.
Keywords: COPD; comorbidity; echocardiography; pulmonary hypertension.
© 2020 Nakayama et al.
Conflict of interest statement
Dr Koichiro Asano reports personal fees from Teijin Pharma Ltd, Novartis Pharma, Sanofi, Astellas Pharma, AstraZeneca, Boehringer-Ingelheim, GlaxoSmithKline, Kyorin Pharma, and MSD, outside the submitted work. The authors report no other conflicts of interest in this work.
Figures
References
-
- Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for the diagnosis, management and prevention of COPD. 2019. Available from: https://goldcopd.org/wp-content/uploads/2018/11/GOLD-2019-v1.7-FINAL-14N.... Accessed March25, 2019.
