

Aortoenteric fistula secondary to an Inflammatory Abdominal Aortic Aneurysm
- PMID: 32184927
- PMCID: PMC7060010
- DOI: 10.3941/jrcr.v13i9.3746
Aortoenteric fistula secondary to an Inflammatory Abdominal Aortic Aneurysm
Abstract
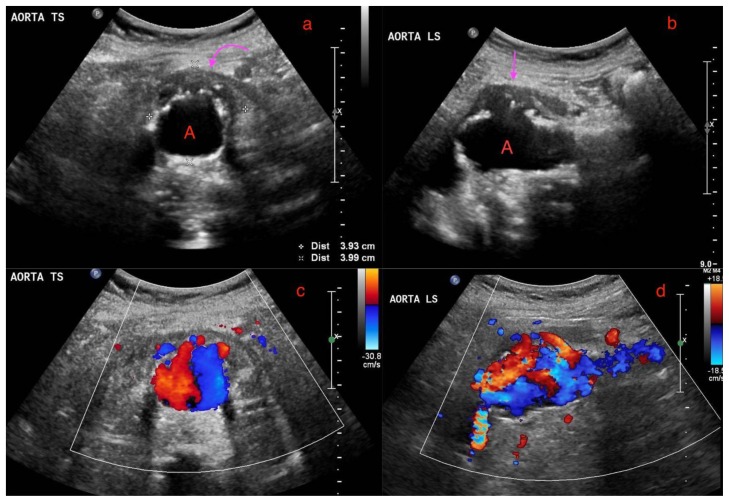
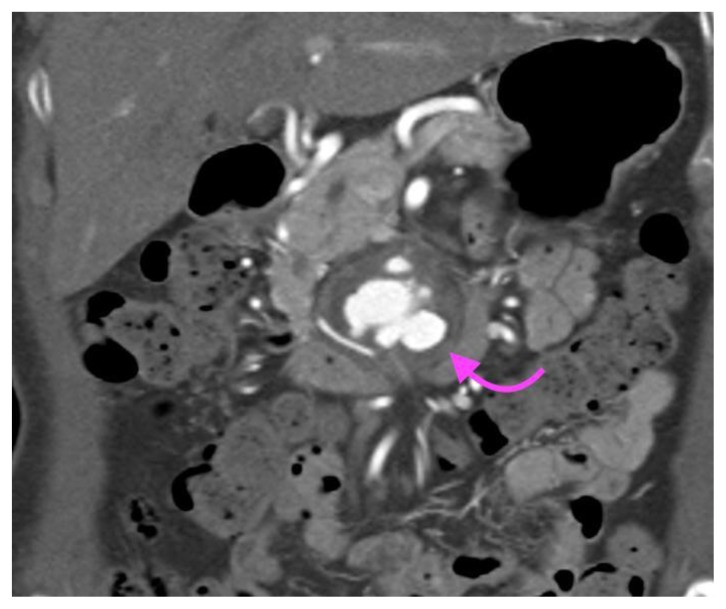
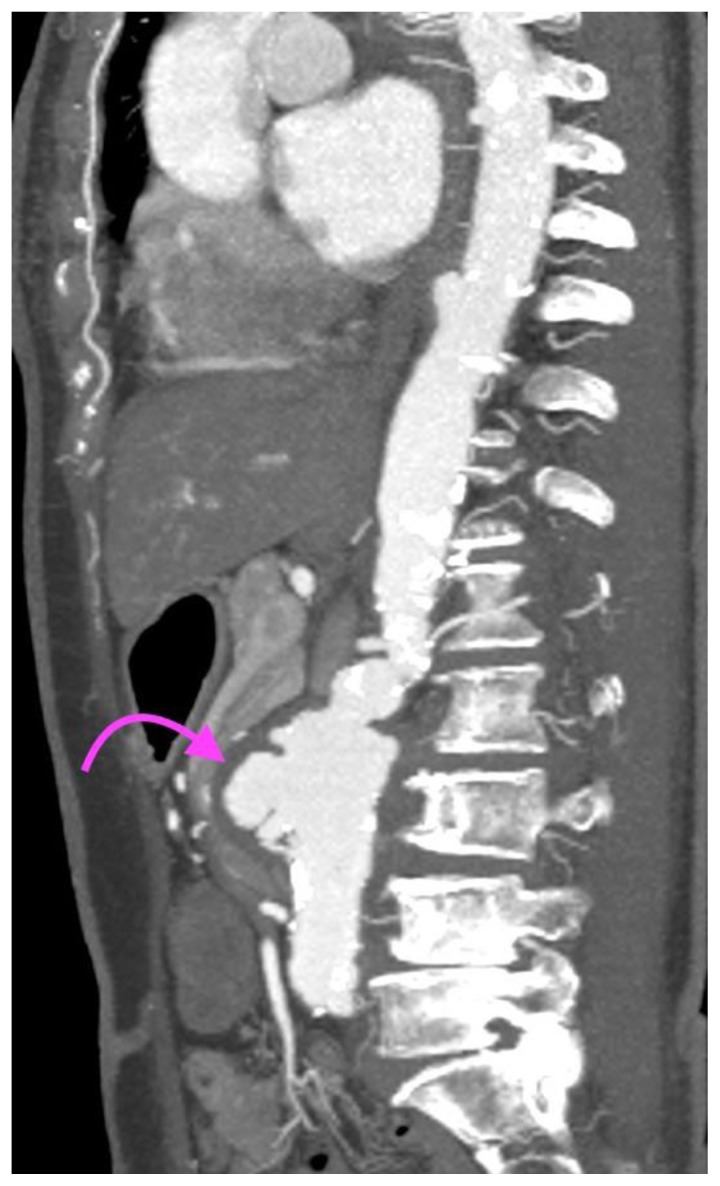
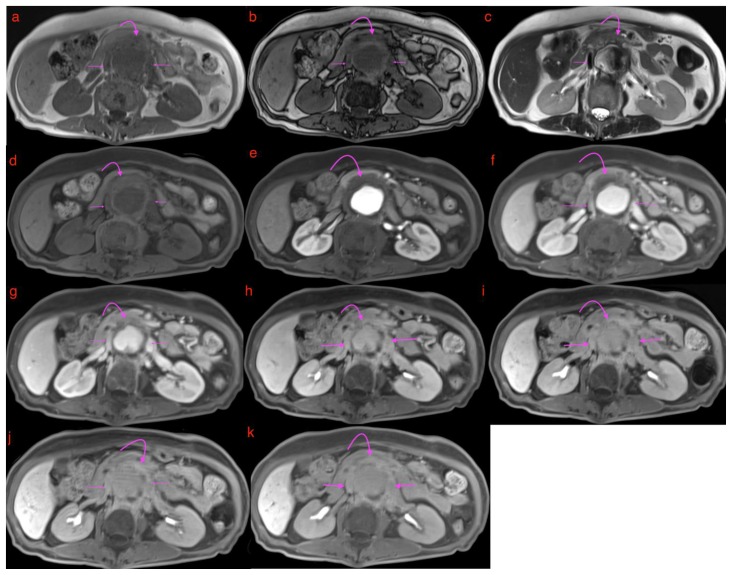
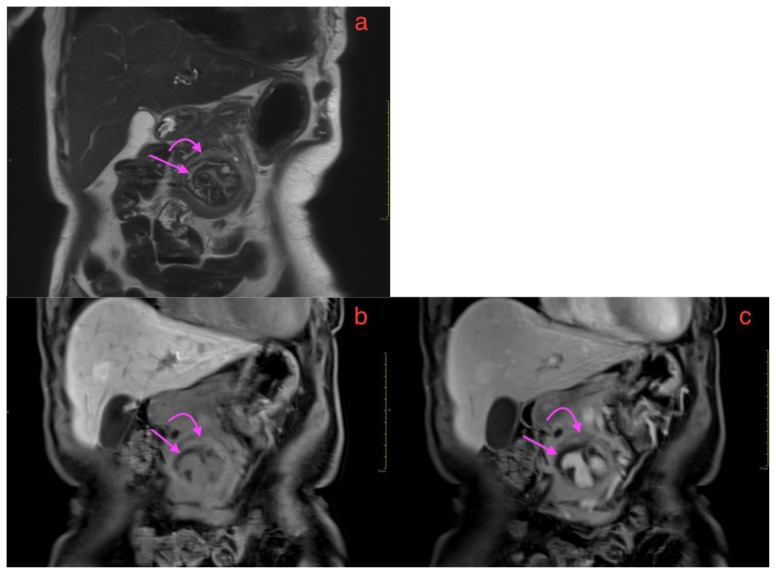
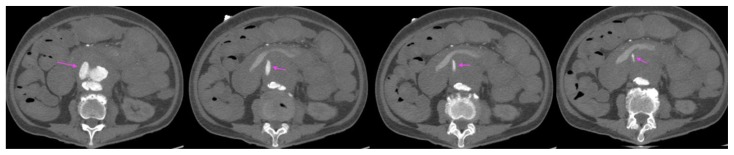
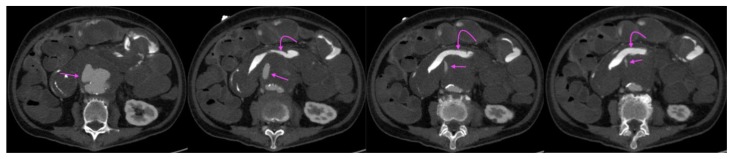
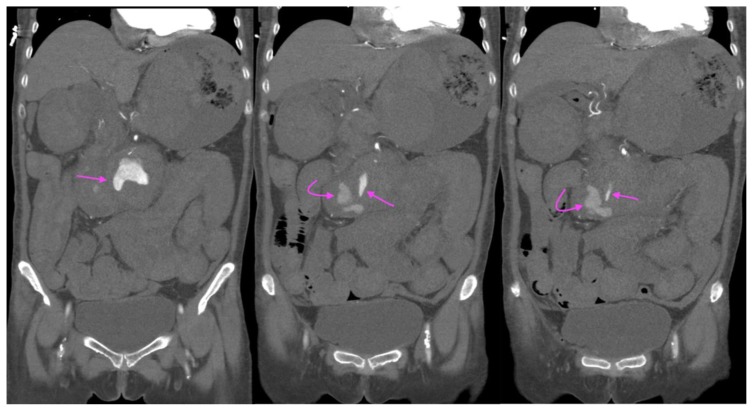
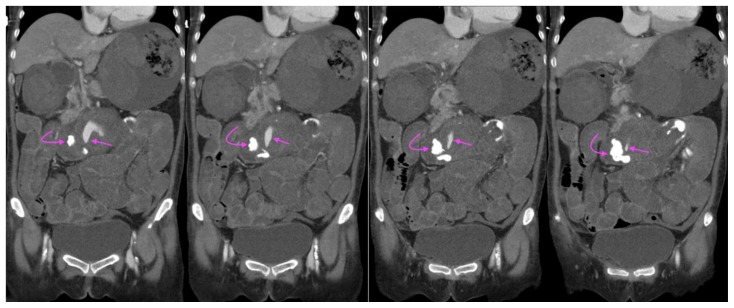
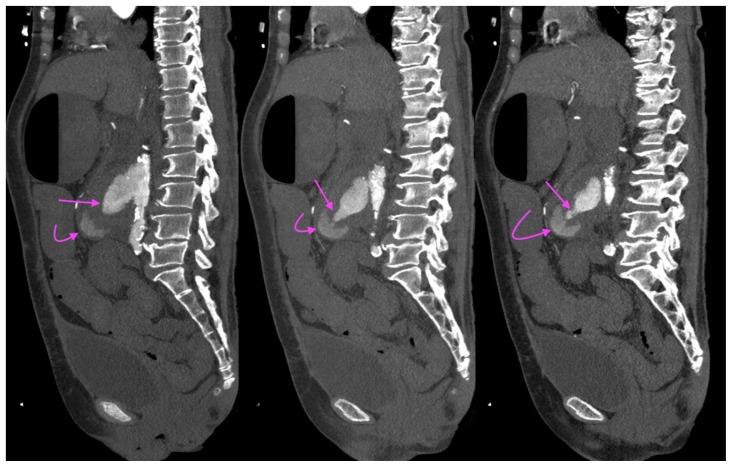
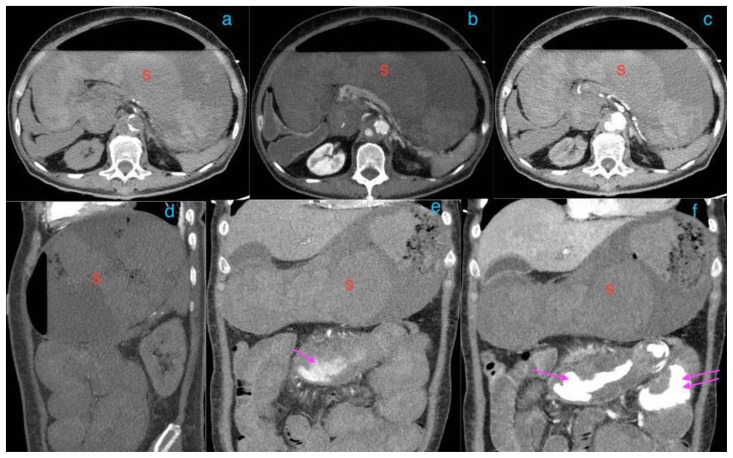
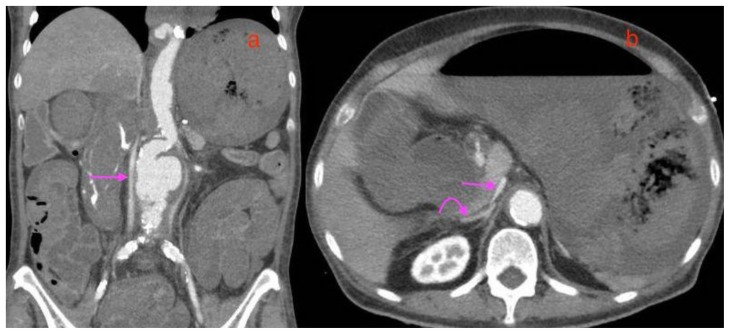
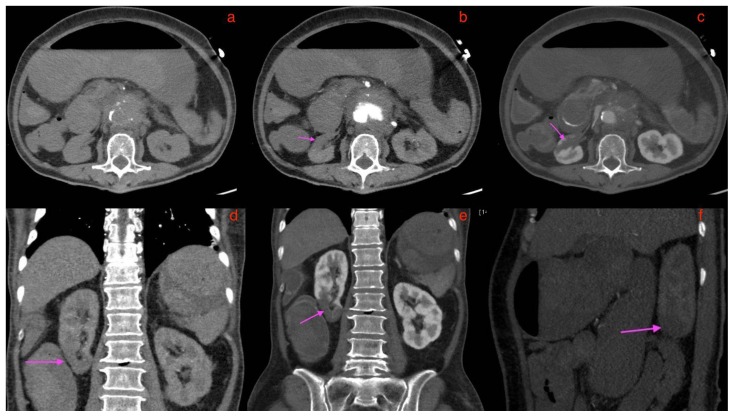
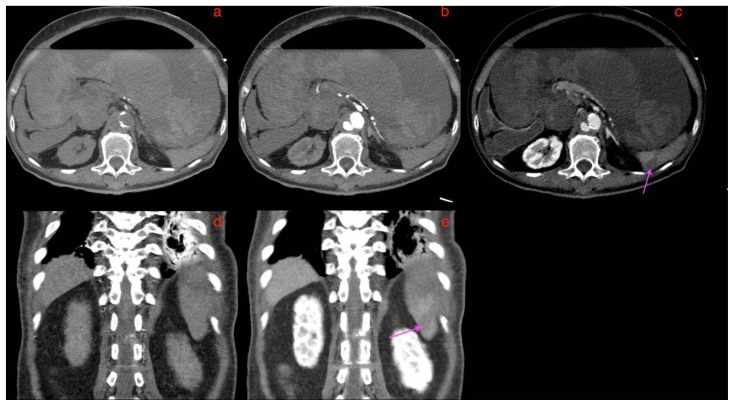
Primary aortoenteric fistulas are rare, with the annual incidence of such fistulas estimated to be 0.007 per million. The most common predisposing conditions for primary aortoenteric fistulas are atherosclerotic abdominal aortic aneurysms or penetrating atherosclerotic ulcers. We illustrate a rare case of an inflammatory aortic aneurysm causing a primary aortic fistula, with a direct fistulous jet from the aorta to the bowel with resultant catastrophic bleeding. In contrast to atherosclerotic aneurysms, most inflammatory aneurysms are symptomatic and show dense perianeurysmal fibrosis and periaortic wall thickening. A direct jet of contrast extravasation from the aorta into a bowel loop, while rarely seen, remains the most specific sign of a primary aorta-enteric fistula. A comprehensive literature review of the clinical presentation, imaging features, and differential diagnosis of a primary aortoenteric fistula are also discussed.
Keywords: Aortoenteric fistula; CT; MRI; abdomen; infectious aortitis; inflammatory abdominal aortic aneurysm; mycotic aneurysm; primary; radiotracer; secondary; ultrasound.
Copyright Journal of Radiology Case Reports.
Figures



References
-
- Tang T, Boyle JR, Dixon AK, Varty K. Inflammatory abdominal aortic aneurysms. Eur J Vasc Endovasc Surg. 2005 Apr;29(4):353–62. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources