

Robotic Inguinal vs Transabdominal Laparoscopic Inguinal Hernia Repair: The RIVAL Randomized Clinical Trial
- PMID: 32186683
- PMCID: PMC7081145
- DOI: 10.1001/jamasurg.2020.0034
Robotic Inguinal vs Transabdominal Laparoscopic Inguinal Hernia Repair: The RIVAL Randomized Clinical Trial
Abstract
Importance: Despite rapid adoption of the robotic platform for inguinal hernia repair in the US, to date, no level I trials have ever compared robotic inguinal hernia repair to laparoscopic repair. This multicenter randomized clinical trial is the first to compare the robotic platform to laparoscopic approach for minimally invasive inguinal hernia repair.
Objective: To determine whether the robotic approach to inguinal hernia repair results in improved postoperative outcomes compared with traditional laparoscopic inguinal hernia repairs.
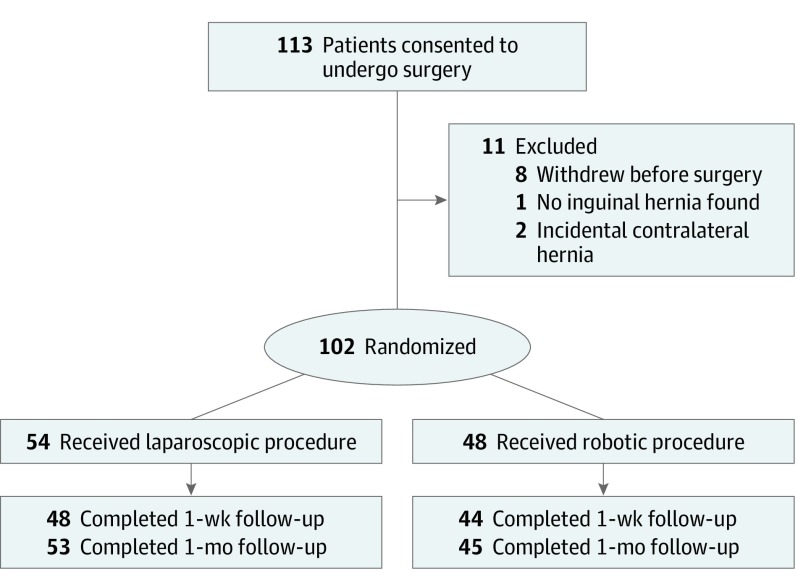
Design, setting, and participants: This multicenter, single-blinded, prospective randomized clinical pilot study was conducted from April 2016 to April 2019, with a follow-up duration of 30 days in 6 academic and academic-affiliated sites. Enrolled in this study were 113 patients with a unilateral primary or recurrent inguinal hernia. After exclusions 102 remained for analysis.
Interventions: Standard laparoscopic transabdominal preperitoneal repair or robotic transabdominal preperitoneal repair.
Main outcomes and measures: Main outcomes included postoperative pain, health-related quality of life, mobility, wound morbidity, and cosmesis. Secondary outcomes included cost, surgeon ergonomics, and surgeon mental workload. A primary outcome was not selected because this study was designed as a pilot study. The hypothesis was formulated prior to data collection.
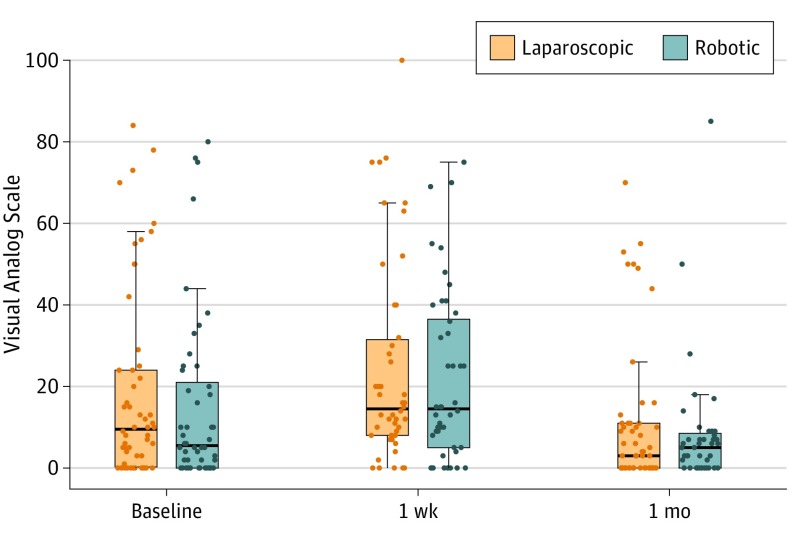
Results: A total of 102 patients were included in the study (54 in the laparoscopic group, mean [SD] age, 57.2 [13.3] years and 48 [88.9%] male; 48 in the robotic group, mean [SD] age, 56.1 [14.1] years and 44 [91.6%] male). There were no differences at the preoperative, 1-week, or 30-day points between the groups in terms of wound events, readmissions, pain as measured by the Visual Analog Scale, or quality of life as measured by the 36-Item Short Form Health Survey. Compared with traditional laparoscopic inguinal hernia repair, robotic transabdominal preperitoneal repair was associated with longer median (interquartile range) operative times (75.5 [59.0-93.8] minutes vs 40.5 [29.2-63.8] minutes, respectively; P < .001), higher median (interquartile range) cost ($3258 [$2568-$4118] vs $1421 [$1196-$1930], respectively; P < .001), and higher mean (SD) frustration levels on the NASA Task Load Index Scale (range, 1-100, with lower scores indicating lower cognitive workload) (32.7 [23.5] vs 20.1 [19.2], respectively; P = .004). There were no differences in ergonomics of the surgeons between the groups as measured by the Rapid Upper Limb Assessment instrument.
Conclusions and relevance: Results of this study showed no clinical benefit to the robotic approach to straightforward inguinal hernia repair compared with the laparoscopic approach. The robotic approach incurred higher costs and more operative time compared with the laparoscopic approach, with added surgeon frustration and no ergonomic benefit to surgeons.
Trial registration: ClinicalTrials.gov Identifier: NCT02816658.
Conflict of interest statement
Figures
Comment in
-
Robotics vs Laparoscopy-Are They Truly Rivals?JAMA Surg. 2020 May 1;155(5):388. doi: 10.1001/jamasurg.2020.0052. JAMA Surg. 2020. PMID: 32186658 No abstract available.
References
-
- Ger R. Laparoscopic hernia operation. Article in German. Chirurg. 1991;62(4):266-270. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
