

The association between anxiety disorders and in-hospital outcomes in patients with myocardial infarction
- PMID: 32187718
- PMCID: PMC7298986
- DOI: 10.1002/clc.23358
The association between anxiety disorders and in-hospital outcomes in patients with myocardial infarction
Abstract
Background: Anxiety disorders are prevalent in patients with myocardial infarction (MI), but the effects of anxiety disorders on in-hospital outcomes within MI patients have not been well studied.
Hypothesis: To examine the effects of concurrent anxiety disorders on in-hospital outcomes in MI patients.
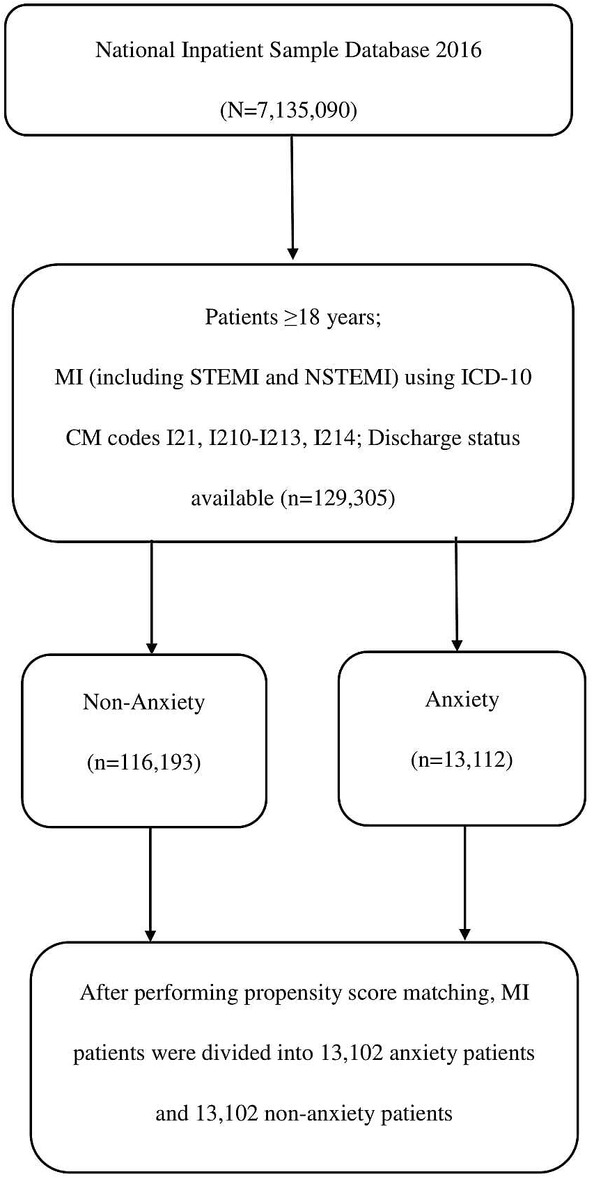
Methods: We conducted a retrospective cohort study in patients with a principal diagnosis of MI with and without anxiety disorders in the National Inpatient Sample 2016. A total of 129 305 primary hospitalizations for acute MI, 35 237 with ST-segment elevation myocardial infarction (STEMI), and 94 068 with non-ST elevation myocardial infarction (NSTEMI) were identified. Of these, 13 112 (10.1%) had anxiety (7.9% in STEMI and 11.0% in NSTEMI). We compared outcomes of anxiety and nonanxiety groups after propensity score matching for the patient and hospital demographics and relevant comorbidities.
Results: After propensity score matching, the anxiety group had a lower incidence of in-hospital mortality (3.0% vs 4.4%, P < .001), cardiac arrest (2.1% vs 2.8%, P < .001), cardiogenic shock (4.9% vs 5.6%, P = .007), and ventricular arrhythmia (6.7% vs 7.9%, P < .001) than the nonanxiety group. In the NSTEMI subgroup, the anxiety group had significantly lower rates of in-hospital mortality (2.3% vs 3.5%, P < .001), cardiac arrest (1.1% vs 1.5%, P = .008), and cardiogenic shock (2.8% vs 3.5%, P = .008). In the STEMI subgroup, we found no differences in in-hospital outcomes (all P > .05) between the matched groups.
Conclusion: Although we found that anxiety was associated with better in-hospital outcomes, subgroup analysis revealed that this only applied to patients admitted for NSTEMI instead of STEMI.
Keywords: anxiety disorders; in-hospital outcomes; myocardial infarction.
© 2020 The Authors. Clinical Cardiology published by Wiley Periodicals, Inc.
Conflict of interest statement
The authors declare no potential conflict of interest.
Figures
References
-
- Roe MT, Messenger JC, Weintraub WS, et al. Treatments, trends, and outcomes of acute myocardial infarction and percutaneous coronary intervention. J Am Coll Cardiol. 2010;56(4):254‐263. - PubMed
-
- Donges K, Schiele R, Gitt A, et al. Incidence, determinants, and clinical course of reinfarction in‐hospital after index acute myocardial infarction (results from the pooled data of the maximal individual therapy in acute myocardial infarction [MITRA], and the myocardial infarction registry [MIR]). Am J Cardiol. 2001;87(9):1039‐1044. - PubMed
-
- Narins CR, Zareba W, Moss AJ, et al. Relationship between intermittent claudication, inflammation, thrombosis, and recurrent cardiac events among survivors of myocardial infarction. Arch Intern Med. 2004;164(4):440‐446. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
