

A ruptured posterior communicating artery aneurysm presenting as tentorial and spinal isolated subdural hemorrhage: a case report and literature review
- PMID: 32188416
- PMCID: PMC7081678
- DOI: 10.1186/s12883-020-01682-8
A ruptured posterior communicating artery aneurysm presenting as tentorial and spinal isolated subdural hemorrhage: a case report and literature review
Abstract
Background: Ruptured intracranial aneurysms are often associated with subarachnoid or intraparenchymal hemorrhage. However, the prevalence of subdural hemorrhage post aneurysmal rupture is low and rarely reported in scientific studies. Here, we report an unusual case of a ruptured posterior communicating artery aneurysm resulting in an isolated subdural hematoma located in the tentorial and spinal canal without subarachnoid or intraparenchymal hemorrhage.
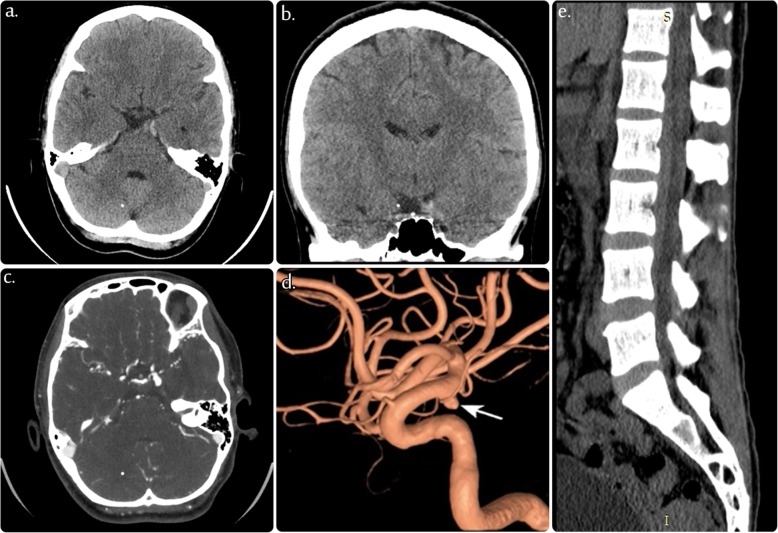
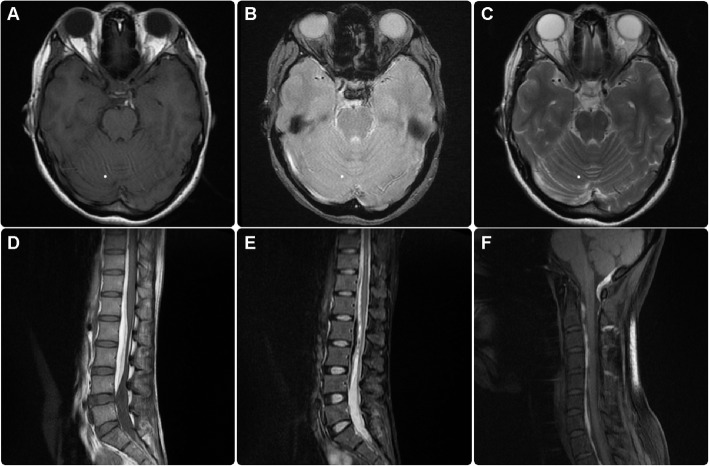
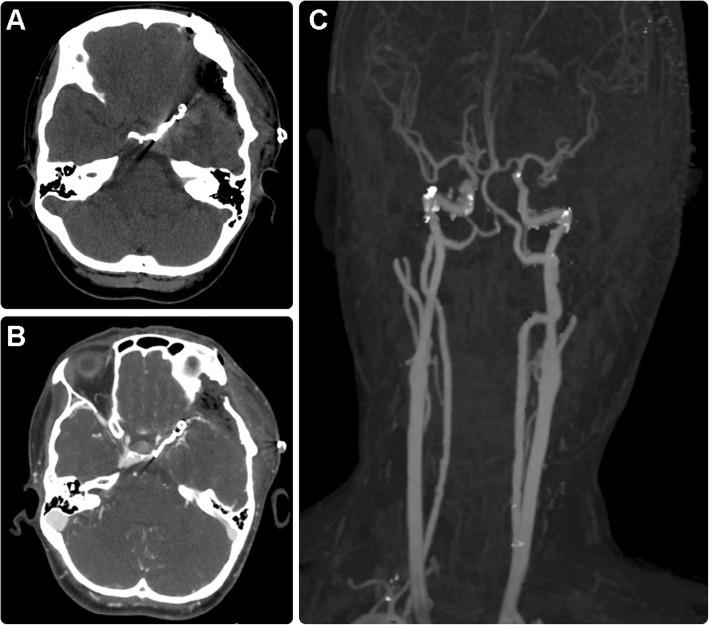
Case presentation: In this case, a 34-year-old woman with no history of trauma or coagulopathy was diagnosed with a subdural hematoma in the tentorium cerebellum tracing to the subdural space of the spinal column. Computed tomography angiography was used to identify the source of the bleeding, which revealed a ruptured left-sided posterior communicating artery saccular aneurysm. The aneurysm was clipped, and the hematoma was evacuated. The patient recovered without any neurological complications.
Conclusions: Our results suggest that a diagnosis of ruptured intracranial aneurysm should be considered in patients with nontraumatic subdural hematoma. Prompt diagnostic imaging and interventional diagnostic procedures are required to ensure proper management of these patients and to avoid unnecessary complications.
Keywords: Clipping; Posterior fossa; Ruptured aneurysm; Saccular aneurysm; Subdural hemorrhage.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures

References
-
- Mrfka M, Pistracher K, Augustin M, Kurschel-Lackner S, Mokry M. Acute subdural hematoma without subarachnoid hemorrhage or intraparenchymal hematoma caused by rupture of a posterior communicating artery aneurysm: case report and review of the literature. J Emerg Med. 2013;44:e369–e373. doi: 10.1016/j.jemermed.2012.11.073. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
