

Impact of concomitant vasoactive treatment and mechanical left ventricular unloading in a porcine model of profound cardiogenic shock
- PMID: 32188462
- PMCID: PMC7079533
- DOI: 10.1186/s13054-020-2816-8
Impact of concomitant vasoactive treatment and mechanical left ventricular unloading in a porcine model of profound cardiogenic shock
Abstract
Background: Concomitant vasoactive drugs are often required to maintain adequate perfusion pressure in patients with acute myocardial infarction (AMI) and cardiogenic shock (CS) receiving hemodynamic support with an axial flow pump (Impella CP).
Objective: To compare the effect of equipotent dosages of epinephrine, dopamine, norepinephrine, and phenylephrine on cardiac work and end-organ perfusion in a porcine model of profound ischemic CS supported with an Impella CP.
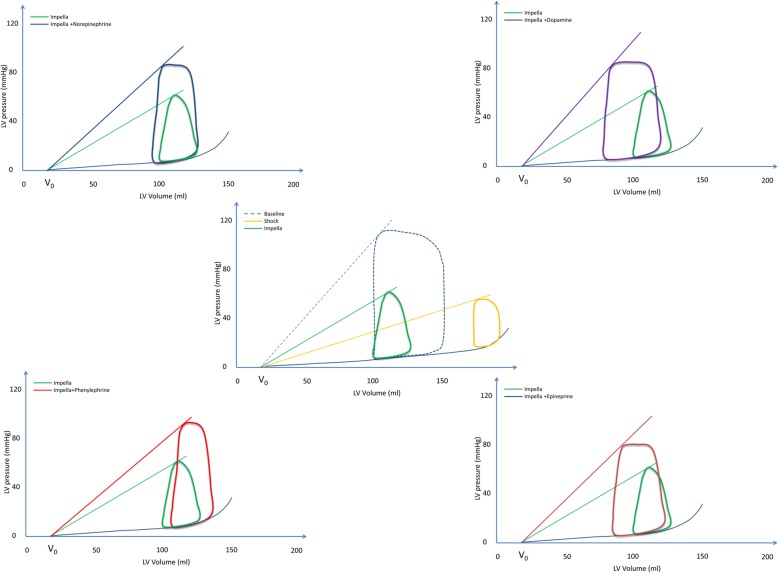
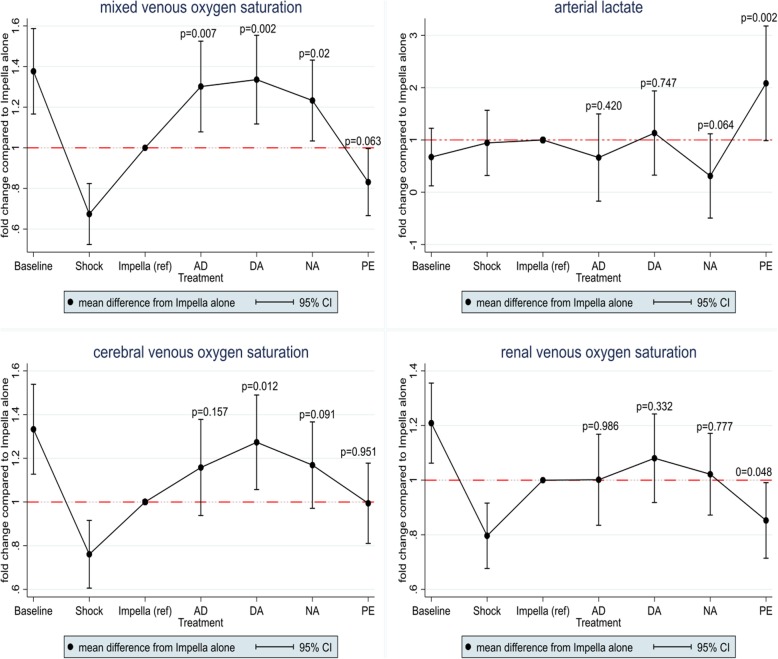
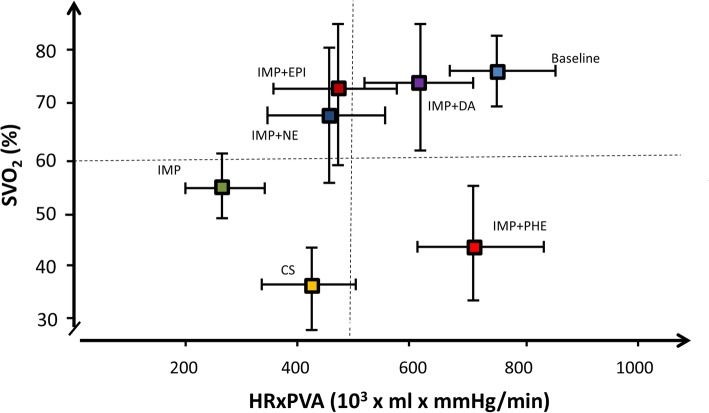
Methods: CS was induced in 10 pigs by stepwise intracoronary injection of polyvinyl microspheres. Hemodynamic support with Impella CP was initiated followed by blinded crossover to vasoactive treatment with norepinephrine (0.10 μg/kg/min), epinephrine (0.10 μg/kg/min), or dopamine (10 μg/kg/min) for 30 min each. At the end of the study, phenylephrine (10 μg/kg/min) was administered for 20 min. The primary outcome was cardiac workload, a product of pressure-volume area (PVA) and heart rate (HR), measured using the conductance catheter technique. End-organ perfusion was assessed by measuring venous oxygen saturation from the pulmonary artery (SvO2), jugular bulb, and renal vein. Treatment effects were evaluated using multilevel mixed-effects linear regression.
Results: All catecholamines significantly increased LV stroke work and cardiac work, dopamine to the greatest extend by 341.8 × 103 (mmHg × mL)/min [95% CI (174.1, 509.5), p < 0.0001], and SvO2 significantly improved during all catecholamines. Phenylephrine, a vasoconstrictor, caused a significant increase in cardiac work by 437.8 × 103 (mmHg × mL)/min [95% CI (297.9, 577.6), p < 0.0001] due to increase in potential energy (p = 0.001), but no significant change in LV stroke work. Also, phenylephrine tended to decrease SvO2 (p = 0.063) and increased arterial lactate levels (p = 0.002).
Conclusion: Catecholamines increased end-organ perfusion at the expense of increased cardiac work, most by dopamine. However, phenylephrine increased cardiac work with no increase in end-organ perfusion.
Keywords: Acute myocardial infarction; Cardiac work; Cardiogenic shock; Mechanical circulatory support; Organ perfusion; Vasopressor.
Conflict of interest statement
The study received a grant from Abiomed. NLJU and OKLH have received travel compensation by Abiomed. JEM has received research grants and speaker’s fee from Abiomed.
Figures
Similar articles
-
Impella RP Versus Pharmacologic Vasoactive Treatment in Profound Cardiogenic Shock due to Right Ventricular Failure.J Cardiovasc Transl Res. 2021 Dec;14(6):1021-1029. doi: 10.1007/s12265-021-10131-x. Epub 2021 May 11. J Cardiovasc Transl Res. 2021. PMID: 33977379
-
Impella CP or VA-ECMO in profound cardiogenic shock: left ventricular unloading and organ perfusion in a large animal model.EuroIntervention. 2019 Feb 8;14(15):e1585-e1592. doi: 10.4244/EIJ-D-18-00684. EuroIntervention. 2019. PMID: 30418160
-
Haemodynamic implications of VA-ECMO vs. VA-ECMO plus Impella CP for cardiogenic shock in a large animal model.ESC Heart Fail. 2024 Aug;11(4):2305-2313. doi: 10.1002/ehf2.14780. Epub 2024 Apr 22. ESC Heart Fail. 2024. PMID: 38649295 Free PMC article.
-
Hemodynamic Support Devices for Shock and High-Risk PCI: When and Which One.Curr Cardiol Rep. 2017 Aug 31;19(10):100. doi: 10.1007/s11886-017-0905-3. Curr Cardiol Rep. 2017. PMID: 28856523 Review.
-
Mechanical circulatory support in cardiogenic shock.Eur Heart J. 2014 Jan;35(3):156-67. doi: 10.1093/eurheartj/eht248. Epub 2013 Sep 7. Eur Heart J. 2014. PMID: 24014384 Review.
Cited by
-
Hemodynamic Effects of Cardiovascular Medications in a Normovolemic and Hemorrhaged Yorkshire-cross Swine Model.Comp Med. 2022 Feb 1;72(1):38-44. doi: 10.30802/AALAS-CM-21-000080. Epub 2021 Dec 7. Comp Med. 2022. PMID: 34876241 Free PMC article.
-
Unloading using Impella CP during profound cardiogenic shock caused by left ventricular failure in a large animal model: impact on the right ventricle.Intensive Care Med Exp. 2020 Aug 12;8(1):41. doi: 10.1186/s40635-020-00326-y. Intensive Care Med Exp. 2020. PMID: 32785808 Free PMC article.
-
Hysteretic device characteristics indicate cardiac contractile state for guiding mechanical circulatory support device use.Intensive Care Med Exp. 2021 Dec 20;9(1):62. doi: 10.1186/s40635-021-00426-3. Intensive Care Med Exp. 2021. PMID: 34928472 Free PMC article.
-
miRNA-200b-A Potential Biomarker Identified in a Porcine Model of Cardiogenic Shock and Mechanical Unloading.Front Cardiovasc Med. 2022 May 25;9:881067. doi: 10.3389/fcvm.2022.881067. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35694659 Free PMC article.
-
Temporary microaxial transvalvular left ventricular assist device for post-myocardial infarction ventricular septal rupture: Bridging a paradigm shift.JTCVS Tech. 2024 Sep 4;28:97-108. doi: 10.1016/j.xjtc.2024.08.019. eCollection 2024 Dec. JTCVS Tech. 2024. PMID: 39669340 Free PMC article.
References
-
- Helgestad OKL, Josiassen J, Hassager C, Jensen LO, Holmvang L, Sørensen A, et al. Temporal trends in incidence and patient characteristics in cardiogenic shock following acute myocardial infarction from 2010 to 2017: a Danish cohort study. Eur J Heart Fail. 2019. 10.1002/ejhf.1566 [Epub ahead of print]. - PubMed
-
- Goldberg RJ, Spencer FA, Gore JM, Lessard D, Yarzebski J. Thirty-year trends (1975 to 2005) in the magnitude of, management of, and hospital death rates associated with cardiogenic shock in patients with acute myocardial infarction a population-based perspective. Circulation. 2009;119(9):1211–1219. - PMC - PubMed
-
- De Luca L, Olivari Z, Farina A, Gonzini L, Lucci D, Di Chiara A, et al. Temporal trends in the epidemiology, management, and outcome of patients with cardiogenic shock complicating acute coronary syndromes. Eur J Heart Fail. 2015;17(11):1124–1132. - PubMed
-
- Rathod KS, Koganti S, Iqbal MB, Jain AK, Kalra SS, Astroulakis Z, et al. Contemporary trends in cardiogenic shock: incidence, intra-aortic balloon pump utilisation and outcomes from the London Heart Attack Group. Eur Heart J Acute Cardiovasc Care. 2018;7(1):16–27. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
