

Assessing oral glucose and intravenous insulin loading protocol in 18F-fluorodeoxyglucose positron emission tomography cardiac viability studies
- PMID: 32190015
- PMCID: PMC7067136
- DOI: 10.4103/wjnm.WJNM_58_18
Assessing oral glucose and intravenous insulin loading protocol in 18F-fluorodeoxyglucose positron emission tomography cardiac viability studies
Abstract
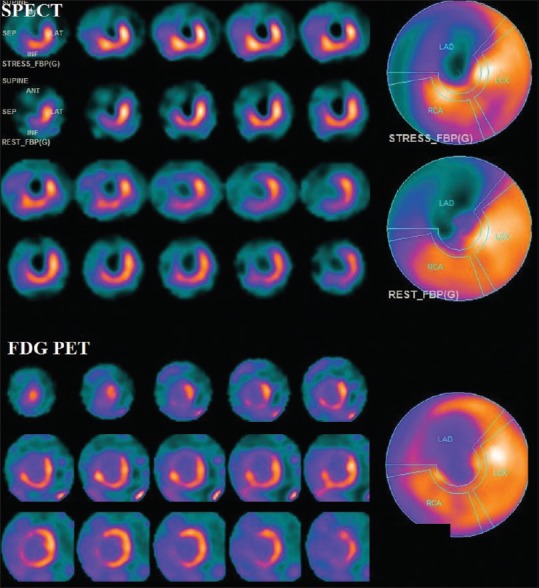
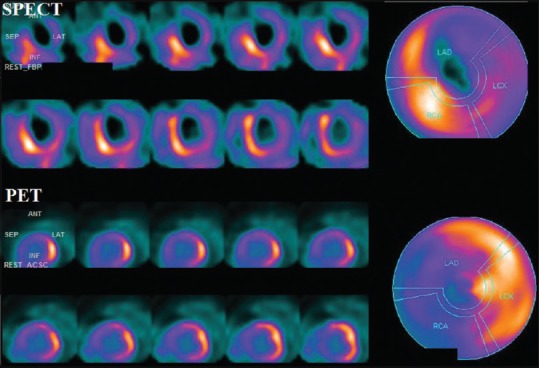
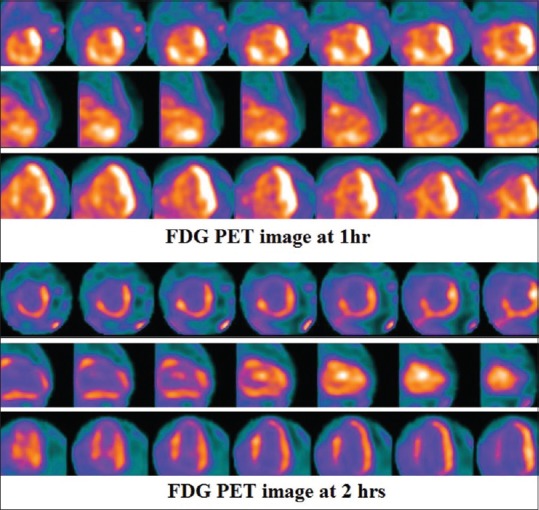
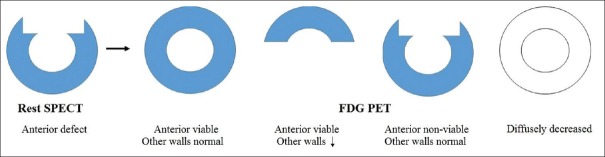
Oral glucose and intravenous insulin (G/I) loading protocols are commonly used in 18F-fluorodeoxyglucose (FDG) positron emission tomography (PET) cardiac viability studies. Although the amount of insulin to be given per blood glucose range has been well described in guidelines, the amount of glucose to be given is not detailed well. In this retrospective study, we aimed to assess if certain parameters, particularly the amount of glucose and insulin given, may affect 18F-FDG uptake in the hibernating myocardium and also determine the problems with this protocol. 18F-FDG PET cardiac viability study with G/I loading protocols was performed in 49 patients. Fasting blood glucose (FBG), amount of glucose given, blood glucose level after glucose load, amount of insulin given, and blood glucose level at the time of 18F-FDG injection were recorded. Statistical analysis was performed to determine if there is any difference in the above values in PET viable and PET nonviable groups and also in subgroups assessing 18F-FDG uptake also in normal myocardium. For G/I loading, we used our local protocol in 43 patients, and other protocols in six. 18F-FDG PET showed viability in 31 patients, and it was negative for viability in 18. In 22 patients, mainly in PET viable group, there was varying degree of reduced 18F-FDG uptake in normal myocardium. There was no significant difference in FBG, amount of glucose given, blood glucose level after glucose load, amount of insulin given, and blood glucose level at the time of 18F-FDG injection in PET viable and PET nonviable groups and also in subgroups. The problems with G/I loading protocol included deciding on the amounts of glucose and insulin given, maximum amount of insulin to be given, handling diabetics, optimal time to measure blood glucose after insulin administration, and interpretation of findings in cases with diffusely reduced 18F-FDG uptake. Further improvements in current guidelines are necessary to obtain images in optimal conditions for accurate results.
Keywords: 18F-fluorodeoxyglucose positron emission tomography; myocardial viability; oral glucose and intravenous insulin loading.
Copyright: © 2020 World Journal of Nuclear Medicine.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- Knuuti MJ, Nuutila P, Ruotsalainen U, Saraste M, Härkönen R, Ahonen A, et al. Euglycemic hyperinsulinemic clamp and oral glucose load in stimulating myocardial glucose utilization during positron emission tomography. J Nucl Med. 1992;33:1255–62. - PubMed
-
- Soares J, Jr, Rodrigues Filho F, Izaki M, Giorgi MC, Catapirra RM, Abe R, et al. Low-carbohydrate diet versus euglycemic hyperinsulinemic clamp for the assessment of myocardial viability with 18F-fluorodeoxyglucose-PET: A pilot study. Int J Cardiovasc Imaging. 2014;30:415–23. - PubMed
-
- Schinkel AF, Bax JJ, Valkema R, Elhendy A, van Domburg RT, Vourvouri EC, et al. Effect of diabetes mellitus on myocardial 18F-FDG SPECT using acipimox for the assessment of myocardial viability. J Nucl Med. 2003;44:877–83. - PubMed
-
- Dilsizian V, Bacharach SL, Beanlands RS, Bergmann SR, Delbeke D, Dorbala S, et al. ASNC imaging guidelines/SNMMI procedure standard for positron emission tomography (PET) nuclear cardiology procedures. J Nucl Cardiol. 2016;23:1187–226. - PubMed
-
- Vitale GD, deKemp RA, Ruddy TD, Williams K, Beanlands RS. Myocardial glucose utilization and optimization of (18) F-FDG PET imaging in patients with non-insulin-dependent diabetes mellitus, coronary artery disease, and left ventricular dysfunction. J Nucl Med. 2001;42:1730–6. - PubMed
LinkOut - more resources
Full Text Sources