

Acupotomy Alleviates Energy Crisis at Rat Myofascial Trigger Points
- PMID: 32190087
- PMCID: PMC7064863
- DOI: 10.1155/2020/5129562
Acupotomy Alleviates Energy Crisis at Rat Myofascial Trigger Points
Abstract
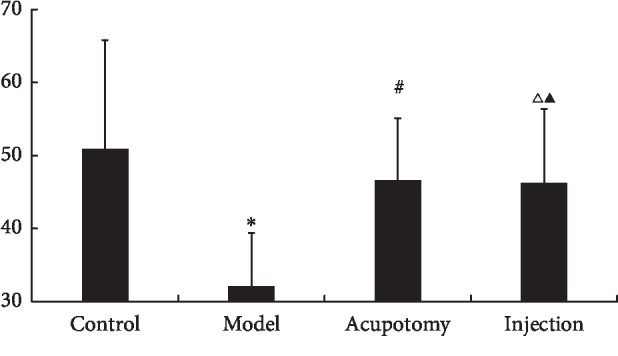
The aim of this study was to determine the effects of acupotomy on energy crises in rat trigger points (TrPs) by measuring mechanical pain thresholds (MPTs) and levels of acetylcholinesterase (AChE), free sarcoplasmic calcium (Ca2+), adenosine 5'-triphosphate (ATP), adenosine 5'-monophosphate (AMP), substance P (SP), and calcitonin gene-related peptide (CGRP) in rat muscle TrP tissue. Male Sprague Dawley rats (n = 32) were randomly divided into four groups: control, TrP, acupotomy, and lidocaine injection. Enzyme-linked immunosorbent assays were used to measure AChE, and free sarcoplasmic Ca2+ concentrations were determined by fluorescent staining with Fura-2 AM; high-performance liquid chromatography was used to measure ATP and AMP, and SP and CGRP were evaluated by immunohistochemistry. Compared with the control group, free sarcoplasmic Ca2+, AMP, SP, and CGRP were higher in the model group, while MPT, AChE, and ATP were lower. Treatment with acupotomy or lidocaine injection reduced free sarcoplasmic Ca2+, SP, and CGRP and increased MPTs and AChE levels compared with the model group. However, only acupotomy also led to decreased AMP and increased ATP levels relative to the model group. We conclude that acupotomy can alleviate energy crises at TrPs.
Copyright © 2020 Yi Zhang et al.
Conflict of interest statement
The authors declare that there are no conflicts of interest regarding the publication of this paper.
Figures







References
-
- Simons D. G., Travell J. Myofascial trigger points, a possible explanation. Pain. 1981;10:106–109. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
