

Facial asymmetry correction: From conventional orthognathic treatment to surgery-first approach
- PMID: 32190216
- PMCID: PMC7072083
- DOI: 10.15171/joddd.2019.047
Facial asymmetry correction: From conventional orthognathic treatment to surgery-first approach
Abstract
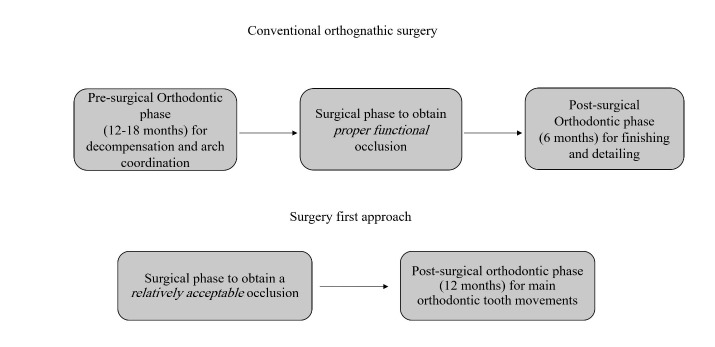
The surgery-first approach (SFA), which proceeds without presurgical orthodontic treatment, is assumed to shorten the treatment course because the direction of post-surgical orthodontic tooth movement conforms to the normal muscular forces. Moreover, the regional acceleratory phenomenon (RAP), evoked by surgery, helps in tooth alignment and compensation in a faster way. Although SFA has definite advantages, especially in class III individuals, there is a lack of data about its indications in patients with facial asymmetry. In this article, we reviewed recently published articles on the treatment of asymmetric patients using the SFA. Different aspects, including the three-dimensional assessment of stability in different planes, approaches for fabrication of a surgical splint, predictability of the results, skills needed for bimaxillary surgery, indications as the treatment of choice for condylar hyperplasia, and combination with distraction osteogenesis in candidates with severe asymmetries were found to be the main topics discussed for patients presenting with facial asymmetry.
Keywords: Surgery first approach; facial asymmetry; orthognathic surgery; skeletal deviation.
© 2019 Hosseinzadeh Nik et al.
References
-
- Proffit WR, White RP, Sarver DM. Contemporary treatment of dentofacial deformity: Mosby ;2003.Chapter 7.Page 254.
-
- Sabri R. Orthodontic objectives in orthognathic surgery: state of the art today. World J Orthod. 2006;7(2) - PubMed
Publication types
LinkOut - more resources
Full Text Sources