

Drug-associated adverse events in the treatment of multidrug-resistant tuberculosis: an individual patient data meta-analysis
- PMID: 32192585
- PMCID: PMC7384398
- DOI: 10.1016/S2213-2600(20)30047-3
Drug-associated adverse events in the treatment of multidrug-resistant tuberculosis: an individual patient data meta-analysis
Abstract
Background: Treatment of multidrug-resistant tuberculosis requires long-term therapy with a combination of multiple second-line drugs. These drugs are associated with numerous adverse events that can cause severe morbidity, such as deafness, and in some instances can lead to death. Our aim was to estimate the absolute and relative frequency of adverse events associated with different tuberculosis drugs to provide useful information for clinicians and tuberculosis programmes in selecting optimal treatment regimens.
Methods: We did a meta-analysis using individual-level patient data that were obtained from studies that reported adverse events that resulted in permanent discontinuation of anti-tuberculosis medications. We used a database created for our previous meta-analysis of multidrug-resistant tuberculosis treatment and outcomes, for which we did a systematic review of literature published between Jan 1, 2009, and Aug 31, 2015 (updated April 15, 2016), and requested individual patient-level information from authors. We also considered for this analysis studies contributing patient-level data in response to a public call made by WHO in 2018. Meta-analysis for proportions and arm-based network meta-analysis were done to estimate the incidence of adverse events for each tuberculosis drug.
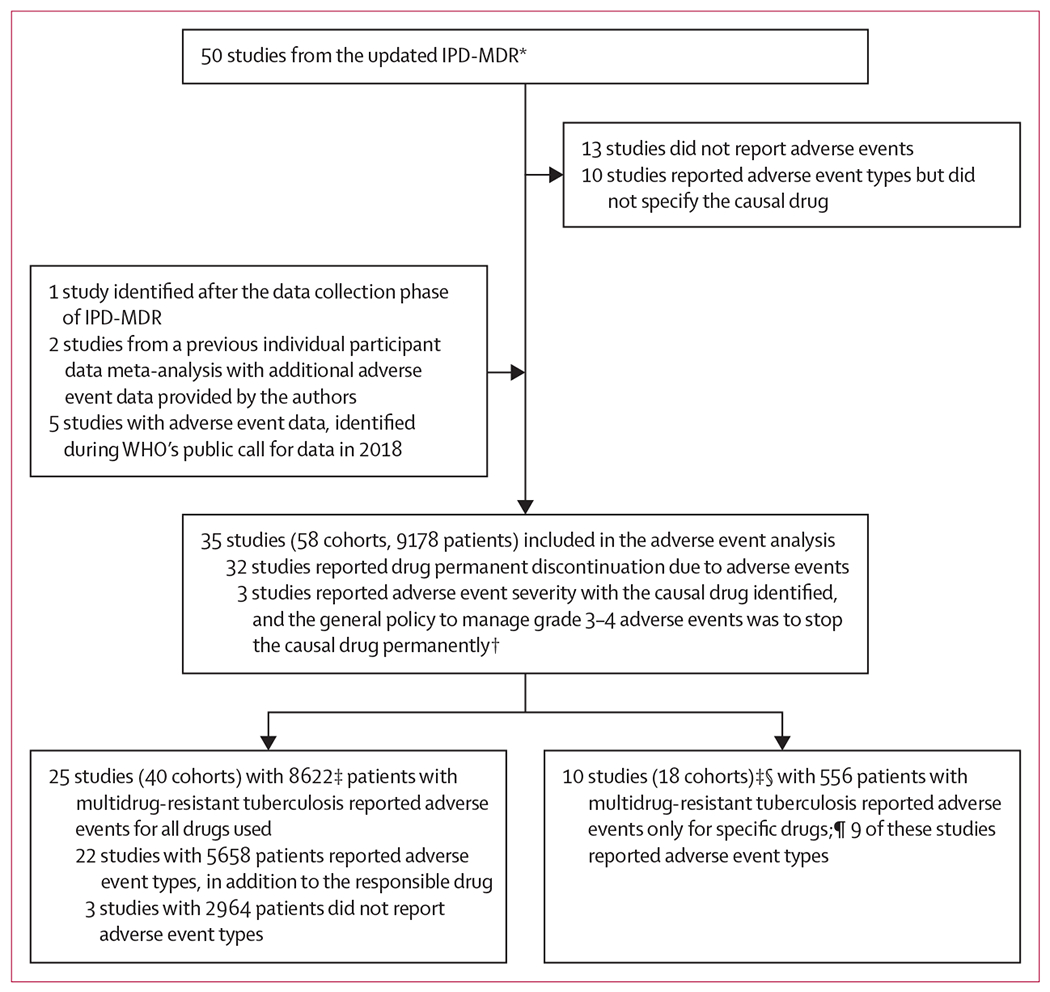
Findings: 58 studies were identified, including 50 studies from the updated individual patient data meta-analysis for multidrug-resistant tuberculosis treatment. 35 of these studies, with 9178 patients, were included in our analysis. Using meta-analysis of proportions, drugs with low risks of adverse event occurrence leading to permanent discontinuation included levofloxacin (1·3% [95% CI 0·3-5·0]), moxifloxacin (2·9% [1·6-5·0]), bedaquiline (1·7% [0·7-4·2]), and clofazimine (1·6% [0·5-5·3]). Relatively high incidence of adverse events leading to permanent discontinuation was seen with three second-line injectable drugs (amikacin: 10·2% [6·3-16·0]; kanamycin: 7·5% [4·6-11·9]; capreomycin: 8·2% [6·3-10·7]), aminosalicylic acid (11·6% [7·1-18·3]), and linezolid (14·1% [9·9-19·6]). Risk of bias in selection of studies was judged to be low because there were no important differences between included and excluded studies. Variability between studies was significant for most outcomes analysed.
Interpretation: Fluoroquinolones, clofazimine, and bedaquiline had the lowest incidence of adverse events leading to permanent drug discontinuation, whereas second-line injectable drugs, aminosalicylic acid, and linezolid had the highest incidence. These results suggest that close monitoring of adverse events is important for patients being treated for multidrug-resistant tuberculosis. Our results also underscore the urgent need for safer and better-tolerated drugs to reduce morbidity from treatment itself for patients with multidrug-resistant tuberculosis.
Funding: Canadian Institutes of Health Research, Centers for Disease Control and Prevention (USA), American Thoracic Society, European Respiratory Society, and Infectious Diseases Society of America.
Copyright © 2020 World Health Organization. Published by Elsevier Ltd. All rights reserved. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests
LB has received personal fees from Ewopharma, and personal fees from Otsuka, outside of the submitted work. CL has received personal fees from Chiesi, and personal fees from Gilead, Janssen, Lucane, Novartis, Oxoid, Berlin Chemie, and Thermofisher, outside of the submitted work. All other authors declare no competing interests.
Figures
References
-
- WHO. Global tuberculosis report 2017. Geneva: World Health Organization, 2017.
-
- WHO. Companion handbook to the WHO guidelines for the programmatic management of drug-resistant tuberculosis. Geneva: World Health Organization, 2014. - PubMed
-
- Wu S, Zhang Y, Sun F, et al. Adverse events associated with the treatment of multidrug-resistant tuberculosis: a systematic review and meta-analysis. Am J Ther 2016; 23: e521–30. - PubMed
-
- Schnippel K, Firnhaber C, Berhanu R, Page-Shipp L, Sinanovic E. Adverse drug reactions during drug-resistant TB treatment in high HIV prevalence settings: a systematic review and meta-analysis. J Antimicrob Chemother 2017; 72: 1871–79. - PubMed
-
- Hwang TJ, Wares DF, Jafarov A, Jakubowiak W, Nunn P, Keshavjee S. Safety of cycloserine and terizidone for the treatment of drug-resistant tuberculosis: a meta-analysis. Int J Tuberc Lung Dis 2013; 17: 1257–66. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
