

Adrenal function after induction therapy for acute lymphoblastic leukemia in children short: adrenal function in ALL
- PMID: 32193656
- PMCID: PMC7413907
- DOI: 10.1007/s00431-020-03624-5
Adrenal function after induction therapy for acute lymphoblastic leukemia in children short: adrenal function in ALL
Abstract
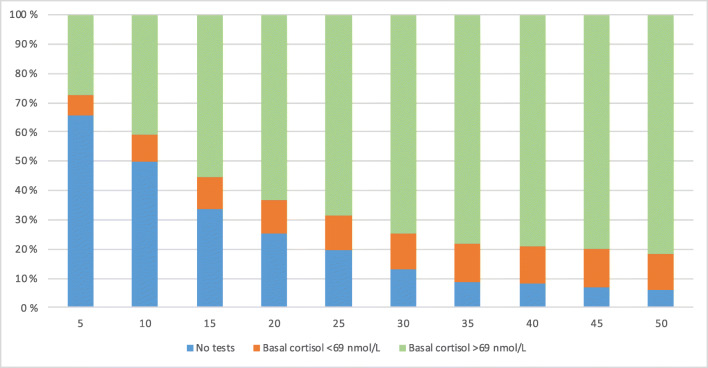
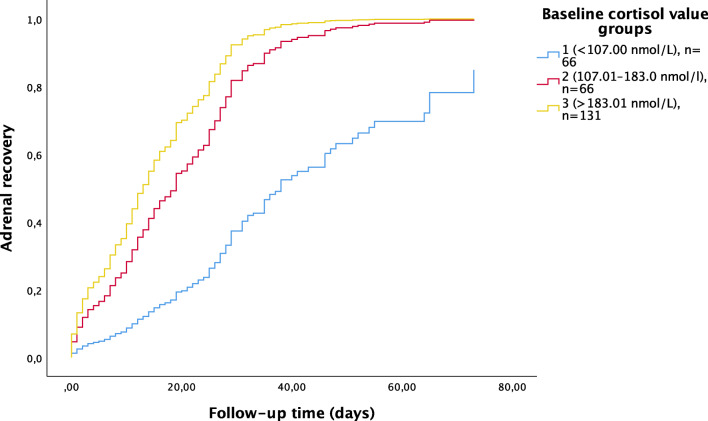
Prednisolone used in the induction phase of the treatment of acute lymphoblastic leukemia (ALL) may suppress hypothalamic-pituitary-adrenal axis and require hydrocortisone substitution. In this retrospective analysis, we reviewed altogether 371 ACTH stimulation tests of 352 children after a uniform NOPHO (Nordic Society of Pediatric Hematology and Oncology) ALL induction. Both low- and standard-dose ACTH tests were used. Full recovery of adrenal function was defined by both normal basal and stimulated cortisol levels. Sixty-two percent of patients were detected with normal adrenal function in median of 15 days after tapering of prednisolone. Both low basal and stimulated cortisol levels were detected in 13% of patients. The median time to normal adrenal function was 31 days (95% CI 28-34), 24 days (95% CI 18-30), and 12 days (95% CI 10-14) for those with basal cortisol <107, 107-183, and >183 nmol/L at first ACTH testing, respectively. Patients with fluconazole prophylaxis had higher median baseline cortisol levels compared to patients without prophylaxis (207 nmol/L, range 21-839 nmol/L vs. 153 nmol/L, range 22-832 nmol/L, P = 0.003).Conclusion: These data can be used to reduce unnecessary substitution or testing, but also to guarantee hydrocortisone substitution for those at risk. What is Known: •These data can be used to reduce unnecessary hydrocortisone substitution or ACTH testing. •Our data helps to guarantee hydrocortisone substitution for those at risk of adrenal insufficiency. What is New: •Full recovery of adrenal function after ALL induction is detected in 62% of patients already at 15 days after tapering of prednisolone. •Both basal and stimulated cortisol testing are required for detection of full adrenal recovery. •Recovery time of adrenal function is extended over 3-4 weeks after tapering of prednisolone in patients with low basal cortisol levels (<107 nmol/L) at first testing.
Keywords: ACTH testing; Acute lymphoblastic leukemia; Adrenal insufficiency; Prednisolone.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures

References
-
- Einaudi S, Bertorello N, Masera N, Farinasso L, Barisone E, Rizzari C, Corrias A, Villa A, Riva F, Saracco P, Pastore G (2008) Adrenal axis function after high-dose steroid therapy for childhood acute lymphoblastic leukemia. Pediatr Blood Cancer. 10.1002/pbc.21339 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
