

Arthroscopic assisted treatment of distal radius fractures and concomitant injuries
- PMID: 32193675
- PMCID: PMC7181439
- DOI: 10.1007/s00402-020-03373-y
Arthroscopic assisted treatment of distal radius fractures and concomitant injuries
Abstract
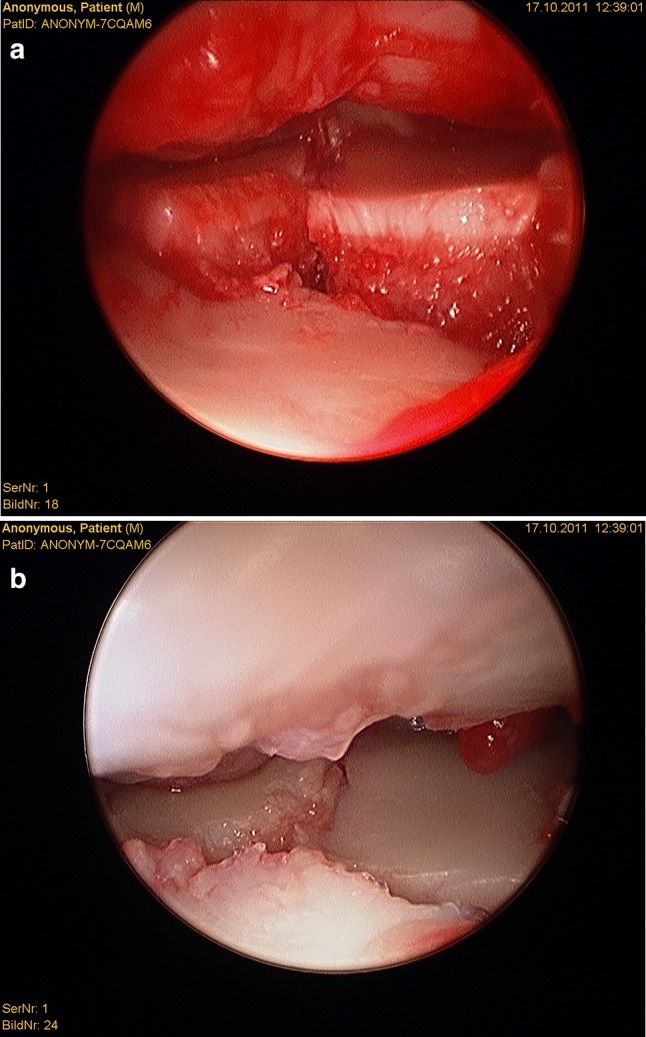
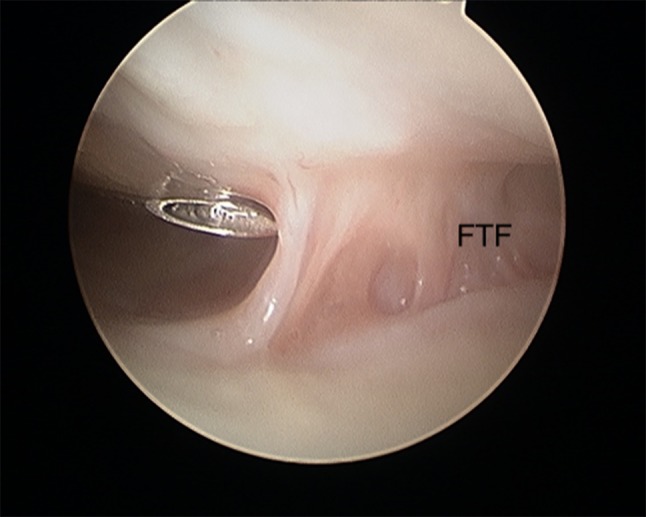
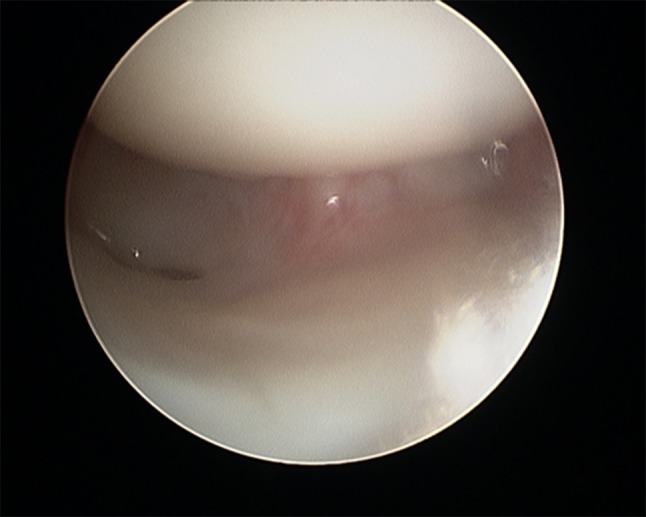
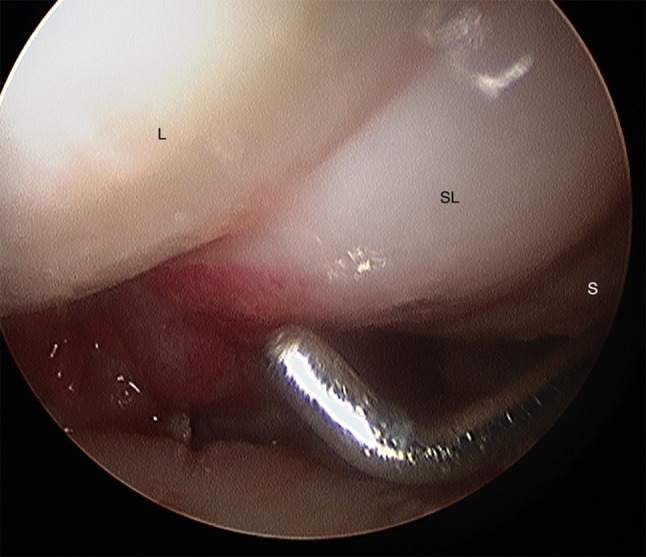
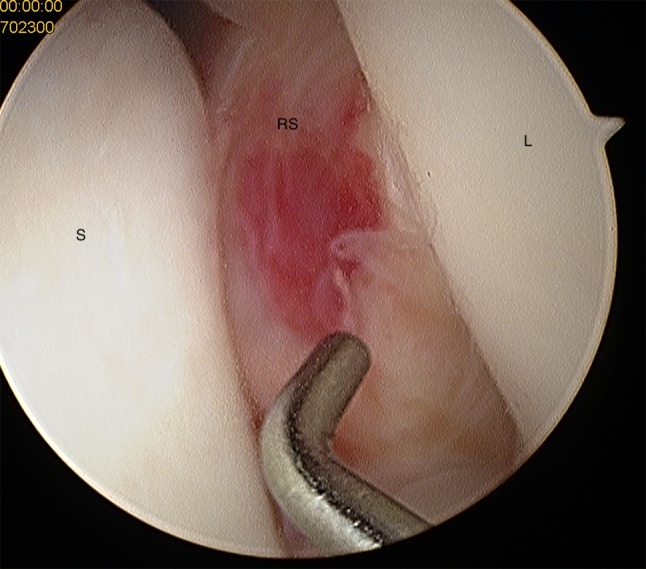
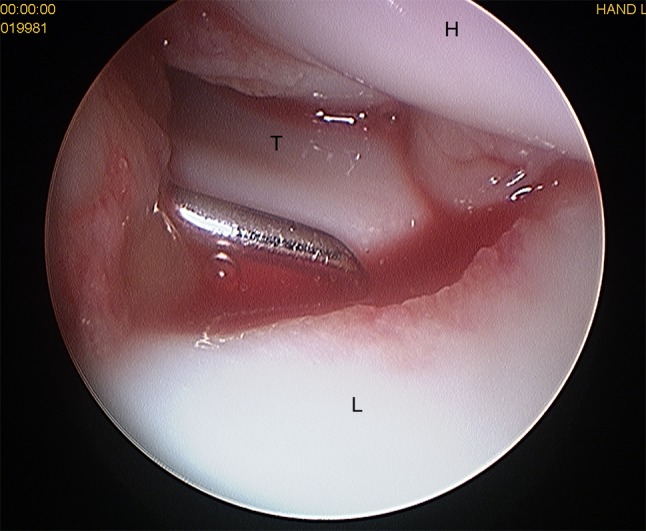
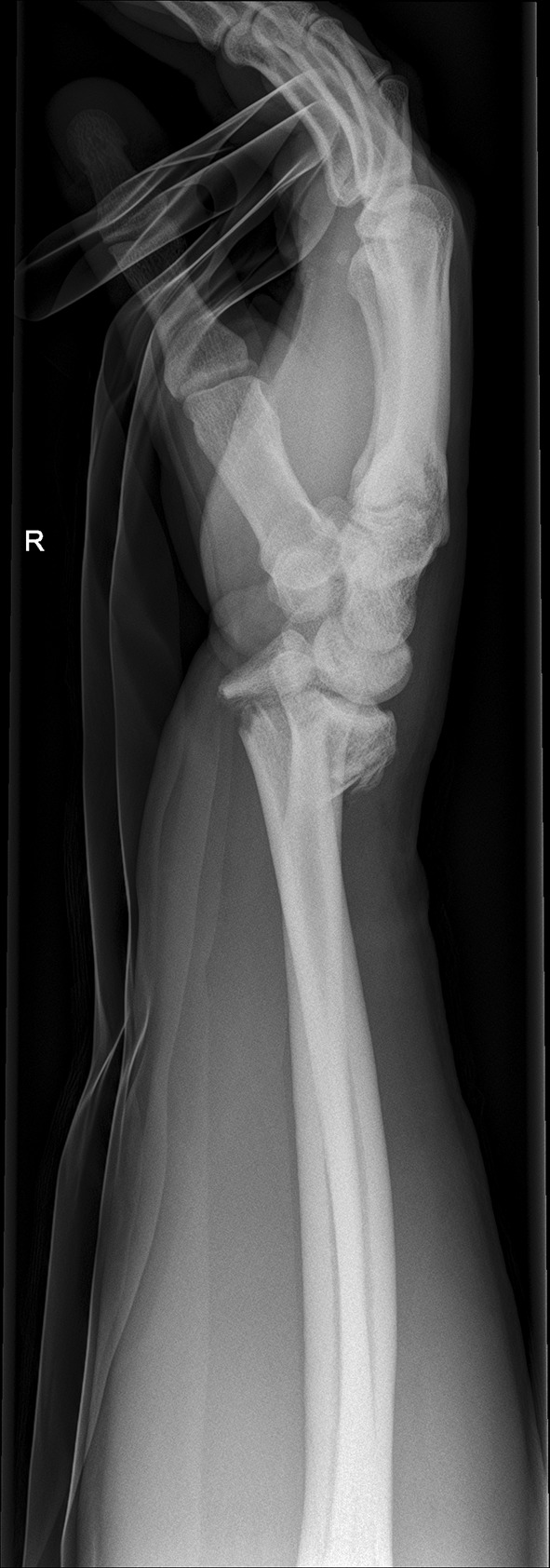
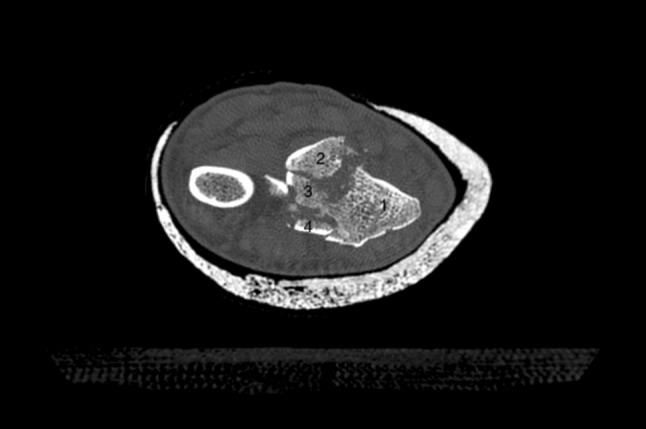
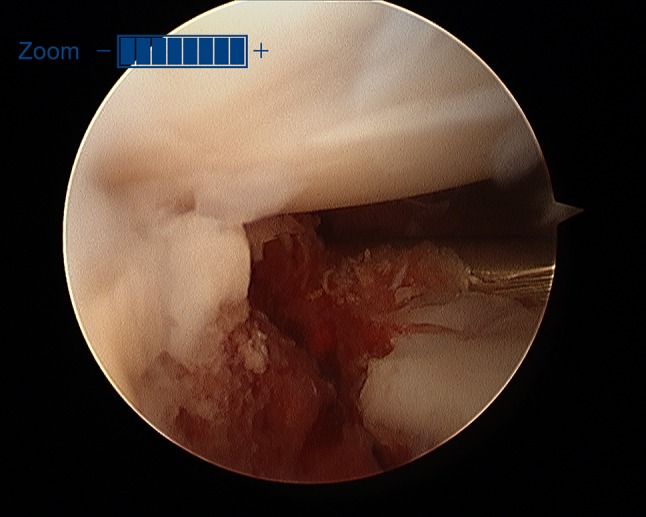
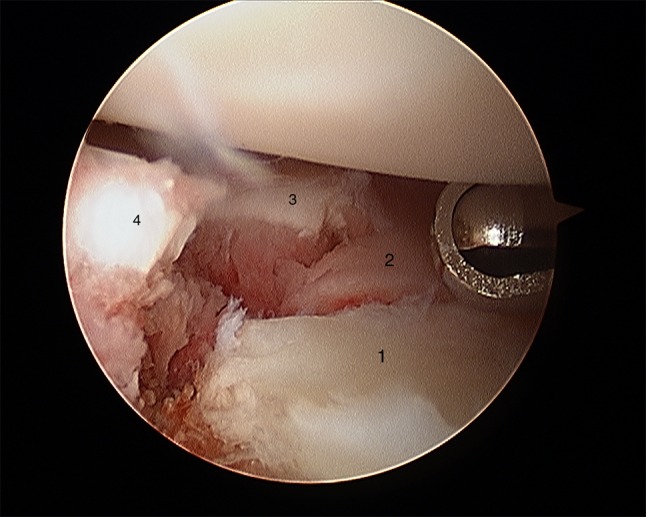
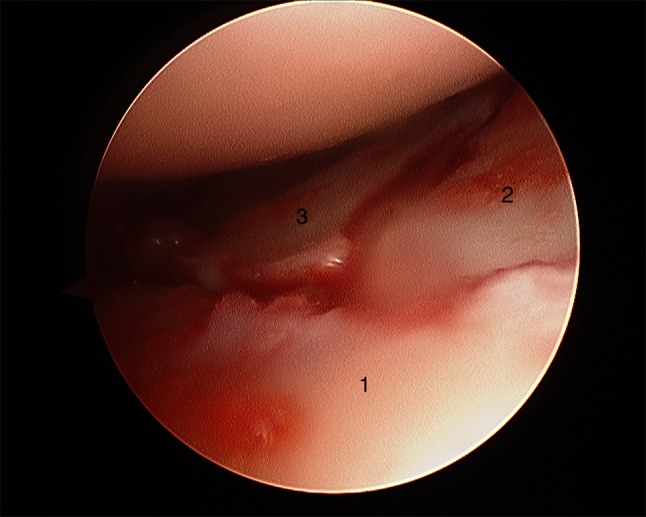
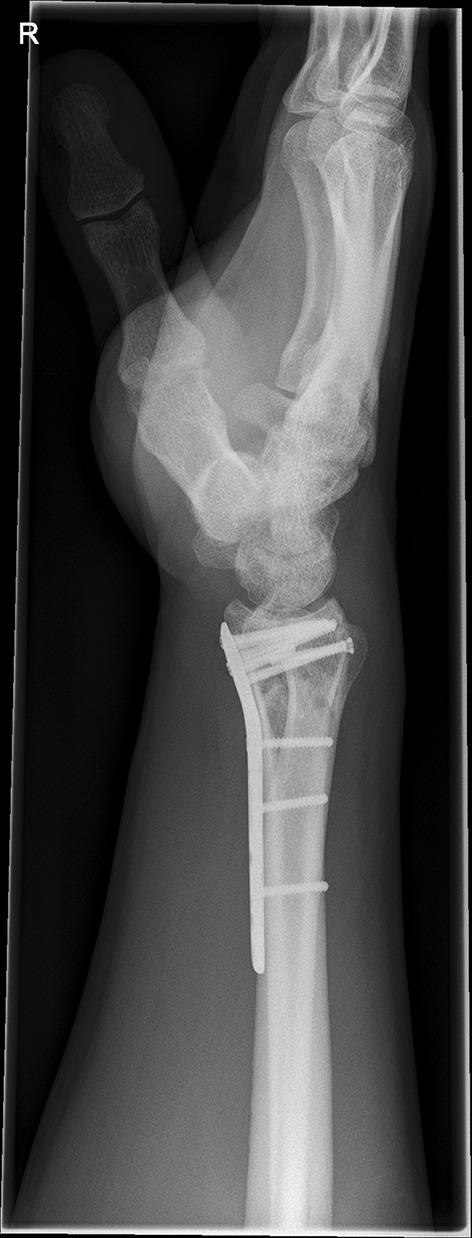
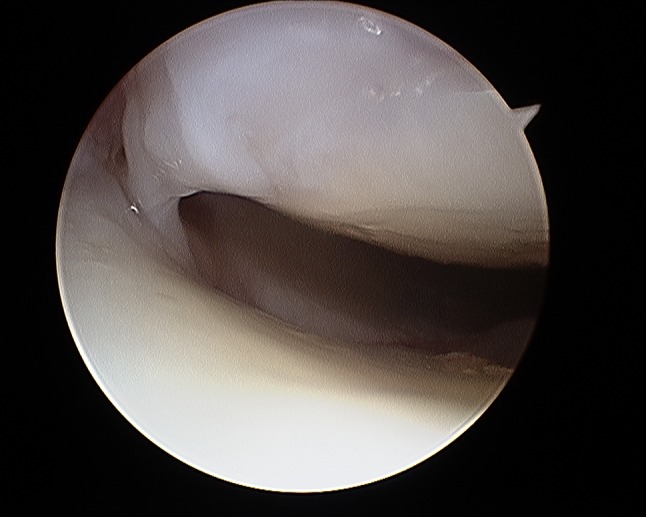
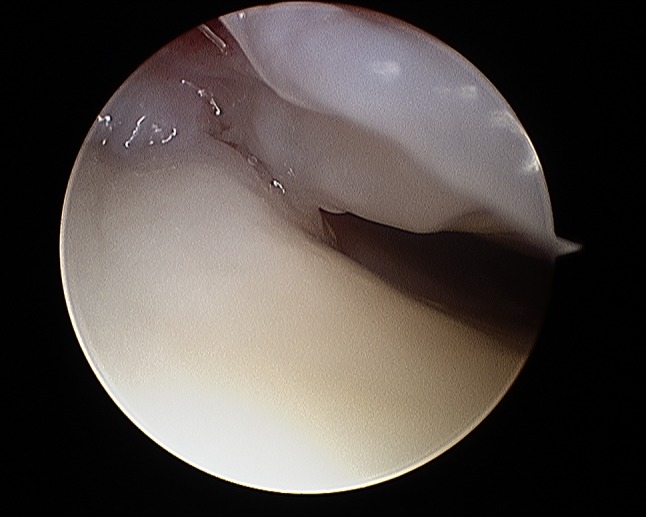
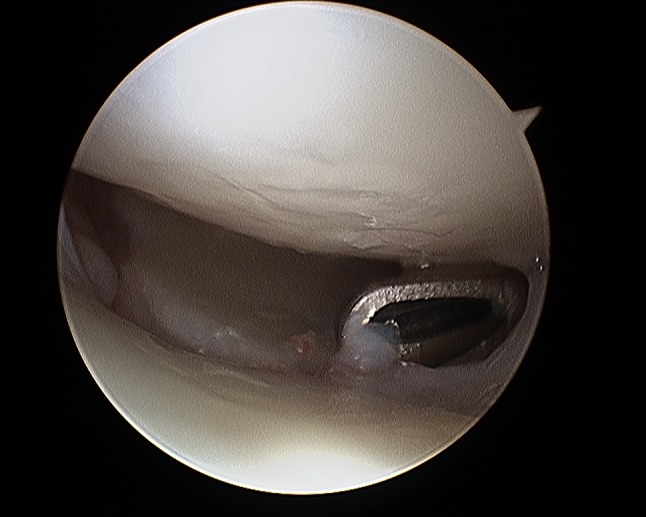
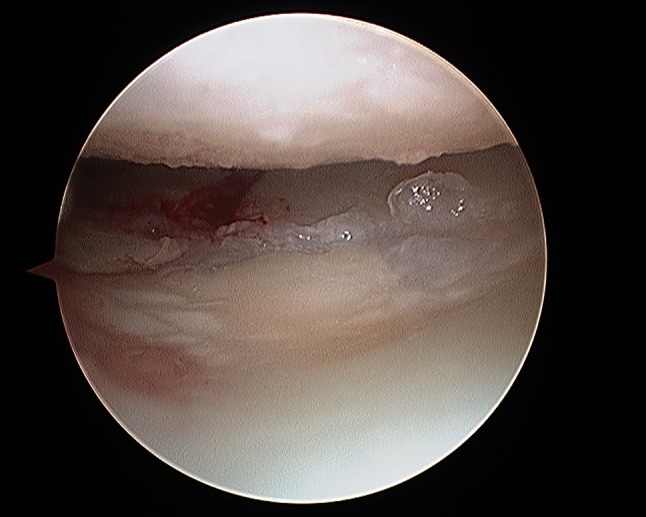
Wrist arthroscopy is mainly used to assist fracture reduction and fixation and to diagnose and treat concomitant injuries mainly to the scapholunate (SL), lunotriquetral (LT) ligament and the triangular fibrocartilage complex (TFCC). Arthroscopy is beneficial in improving anatomical reduction of fracture steps and gaps in intra-articular distal radius fractures (DRFs). Yet, the literature that the functional outcome correlates with the use of arthroscopy, is limited. Non-surgical treatment and immobilization is recommended for Geissler grade I-III Sl-ligament injuries, while open reduction, ligament suture and/or K-wire pinning is mandatory for complete ligament tears according to Geissler grade IV. This manuscript describes the current literature and gives insight into the authors' opinions and practice.
Keywords: Arthroscopic treatment; Concomitant injuries; Distal radius fracture; Injury; Intrinsic ligament.
Conflict of interest statement
No author has a conflict of interest that relates to the content discussed in this manuscript. None of the authors’ professional or financial affiliations that may be perceived as having biased the manuscript. Each author certifies that he or she, or a member of their immediate family, has no commercial associations (i.e., consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article.
Figures















References
-
- Koval KJ, Harrast JJ, Anglen JO, Weinstein JN. Fractures of the distal part of the radius. The evolution of practice over time. Where's the evidence? J Bone Jt Surg Am. 2008;90(9):1855–1861. - PubMed
-
- Atesok K, Doral MN, Whipple T, Mann G, Mei-Dan O, Atay OA, et al. Arthroscopy-assisted fracture fixation. Knee Surg Sports Traumatol Arthrosc. 2011;19(2):320–329. - PubMed
-
- Dei Giudici L, Di Muzio F, Bottegoni C, Chillemi C, Gigante A. The role of arthroscopy in articular fracture management: the lower limb. Eur J Orthop Surg Traumatol. 2015;25(5):807–813. - PubMed
-
- Smeraglia F, Del Buono A, Maffulli N. Wrist arthroscopy in the management of articular distal radius fractures. Br Med Bull. 2016;119(1):157–165. - PubMed
-
- Ardouin L, Durand A, Gay A, Leroy M. Why do we use arthroscopy for distal radius fractures? Eur J Orthop Surg Traumatol. 2018;28(8):1505–1514. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
