

Risk factors predicting less favorable outcomes in endoscopic lumbar discectomies
- PMID: 32195424
- PMCID: PMC7063323
- DOI: 10.21037/jss.2019.11.04
Risk factors predicting less favorable outcomes in endoscopic lumbar discectomies
Abstract
Background: Endoscopic lumbar discectomy was among the first minimally invasive spine procedures commonly performed. As such, all the benefits of minimal invasion were seen, including less pain, less soft tissue destruction, and faster recovery. While outcomes compare favorably to micro and open discectomy, not all patients fare equally well. This paper examines independent risk factors to assess their correlation to suboptimal outcomes after endoscopic lumbar discectomy.
Methods: Retrospective analysis of clinical outcomes of 55 consecutive patients treated with endoscopic discectomy between June 2018 and March 2019 by the author. Primary outcome measures were postoperative reductions of visual analog score (VAS) for back and leg pain modified MacNab criteria as well as time to narcotic independence. Risk factors examined included smoking, facet disease, adjacent segments disc degeneration, obesity, alcohol abuse, and psychiatric illness.
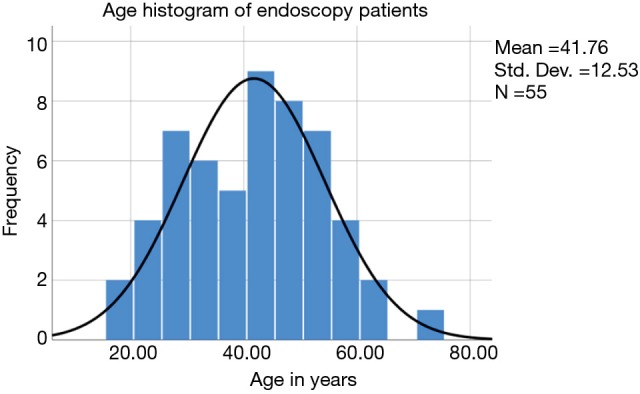
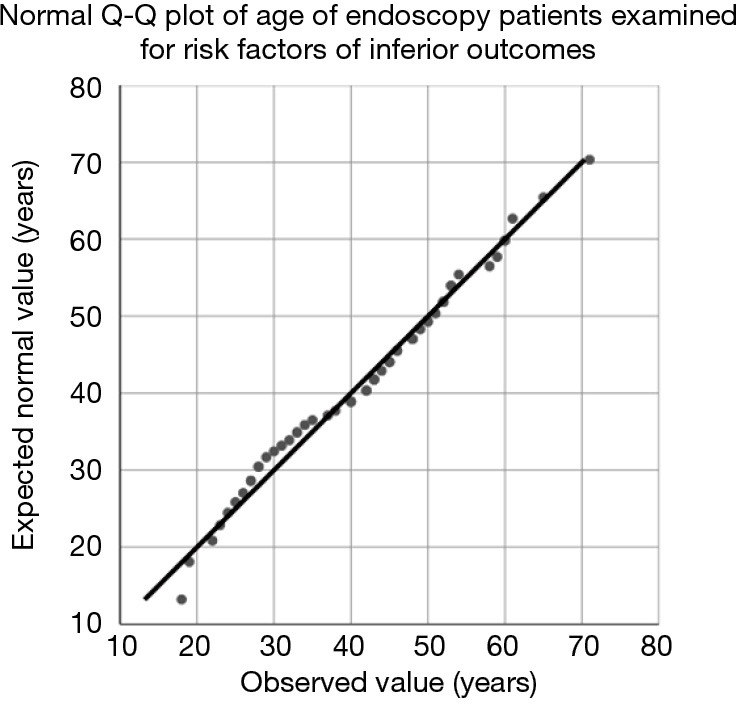
Results: There were 31 males and 24 females with a mean age of 41.76±12.53. Most patients suffered from contained herniations (49.1%) followed by extruded herniations (18.2%). Follow-up ranged from 6-18 months. The most common surgical levels were L5-S1 level (30.9%), L4-S1 (29.1%), and L4-5 (25.5%). The mean return to work (RTW) was 23.83±26.01 weeks. The average body mass index (BMI) was 29.11±4.75. The average time for narcotic independence was 9.64±7.29 days. MacNab outcomes showed that 47.3% (26/55) had excellent, 36.4% good (20/55), 12.7% fair (7/55), and 3.6% had poor (2/55), respectively. The VAS scores for the back (7.69 to 2.65) and leg (6.78 to 2.65) pain reduced significantly (P<0.0001). Smoking (P=0.048), psychiatric disease (P=0.029), disc herniations larger than 10 mm, facet disease, obesity (BMI >30), diabetes, and alcohol abuse was associated with fair and poor MacNab outcomes.
Conclusions: Endoscopic lumbar discectomy safely and reliably reduces axial pain and radiculopathy from lumbar disc herniations. Risk factors associated with incomplete pain relief are large herniations, obesity, instability, smoking, advanced facet degeneration, and decreased ability to cope with the surgery.
Keywords: Endoscopic discectomy; outcome; risk factors.
2020 Journal of Spine Surgery. All rights reserved.
Conflict of interest statement
Conflicts of Interest: The author has no conflicts of interest to declare.
Figures
References
LinkOut - more resources
Full Text Sources