

Shared mechanisms of multimorbidity in COPD, atherosclerosis and type-2 diabetes: the neutrophil as a potential inflammatory target
- PMID: 32198215
- PMCID: PMC9488696
- DOI: 10.1183/16000617.0102-2019
Shared mechanisms of multimorbidity in COPD, atherosclerosis and type-2 diabetes: the neutrophil as a potential inflammatory target
Abstract
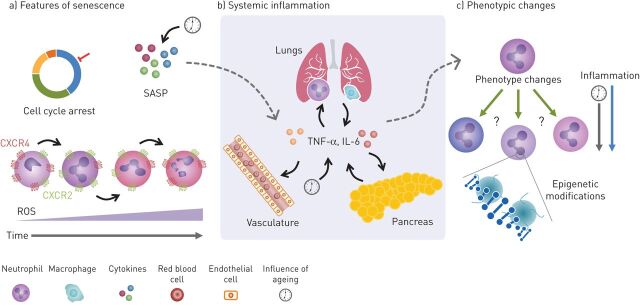
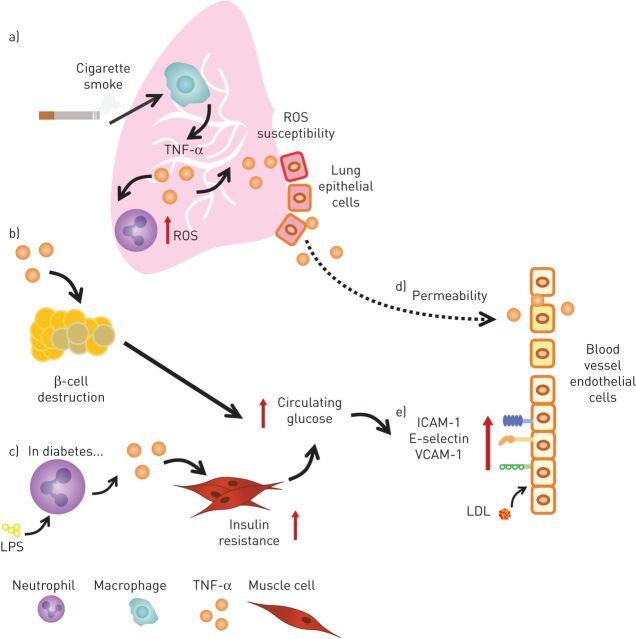
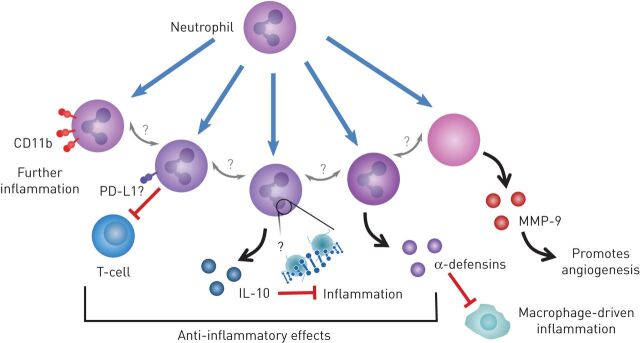
Multimorbidity is increasingly common and current healthcare strategies are not always aligned to treat this complex burden of disease. COPD, type-2 diabetes mellitus (T2D) and cardiovascular disease, especially atherosclerosis, occur more frequently together than expected, even when risk factors such as smoking, obesity, inactivity and poverty are considered. This supports the possibility of unifying mechanisms that contribute to the pathogenesis or progression of each condition.Neutrophilic inflammation is causally associated with COPD, and increasingly recognised in the pathogenesis of atherosclerosis and T2D, potentially forming an aetiological link between conditions. This link might reflect an overspill of inflammation from one affected organ into the systemic circulation, exposing all organs to an increased milieu of proinflammatory cytokines. Additionally, increasing evidence supports the involvement of other processes in chronic disease pathogenesis, such as cellular senescence or changes in cellular phenotypes.This review explores the current scientific evidence for inflammation, cellular ageing and cellular processes, such as reactive oxygen species production and phenotypic changes in the pathogenesis of COPD, T2D and atherosclerosis; highlighting common mechanisms shared across these diseases. We identify emerging therapeutic approaches that target these areas, but also where more work is still required to improve our understanding of the underlying cellular biology in a multimorbid disease setting.
Copyright ©ERS 2020.
Conflict of interest statement
Conflict of interest: M.J. Hughes reports grants from Wellcome Trust, during the conduct of the study. Conflict of interest: H.M. McGettrick has nothing to disclose. Conflict of interest: E. Sapey reports grants from Wellcome Trust, British Lung Foundation, Medical Research Council, NIHR and Dunhill Trust, outside the submitted work.
Figures
References
-
- Lee CTC, Mao IC, Lin CH, et al. Chronic obstructive pulmonary disease: a risk factor for type 2 diabetes. A nationwide population-based study. Eur J Clin Invest 2013; 43: 1113–1119. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical