

Confirmation of 123I-FP-CIT SPECT Quantification Methods in Dementia with Lewy Bodies and Other Neurodegenerative Disorders
- PMID: 32198310
- PMCID: PMC9364894
- DOI: 10.2967/jnumed.119.239418
Confirmation of 123I-FP-CIT SPECT Quantification Methods in Dementia with Lewy Bodies and Other Neurodegenerative Disorders
Abstract
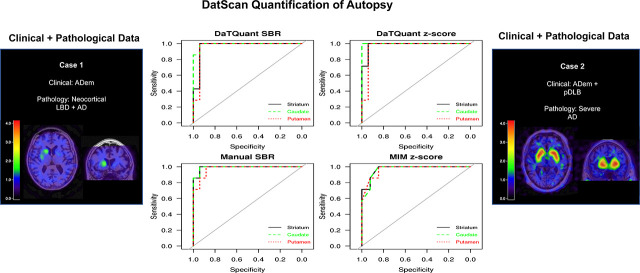
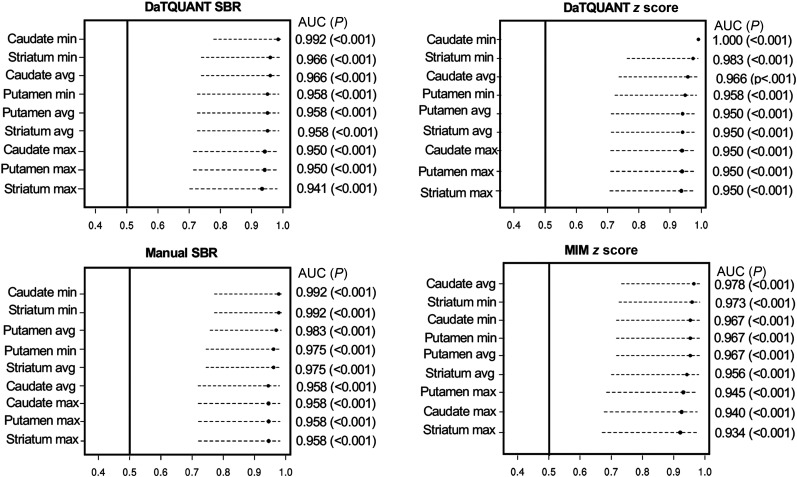
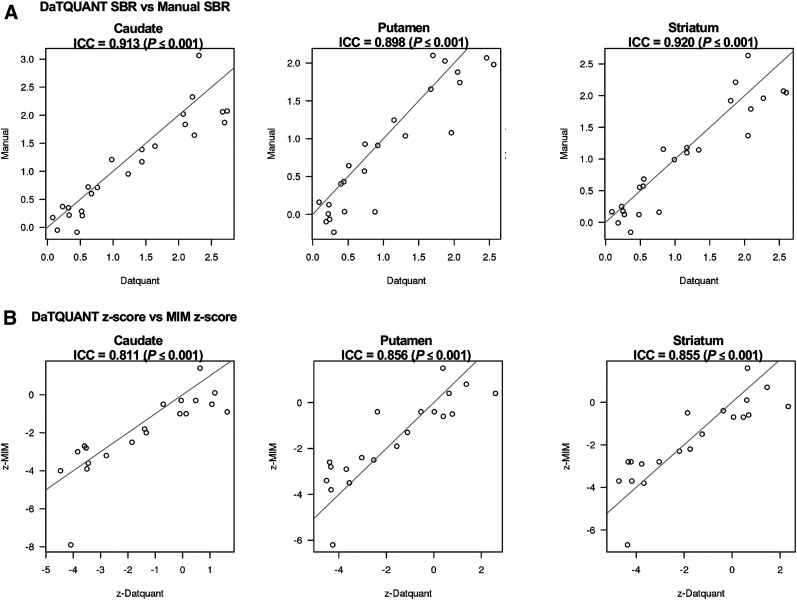
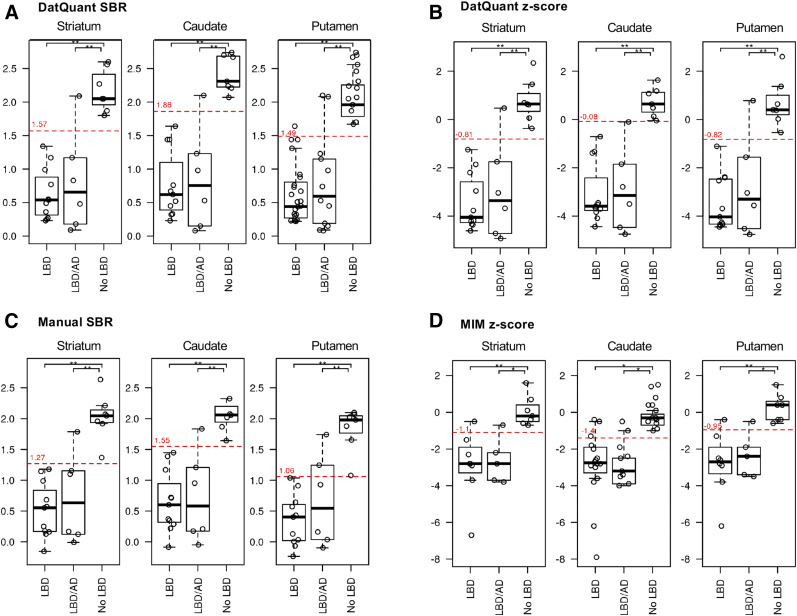
Our rationale was to conduct a retrospective study comparing 3 123I-N-ω-fluoropropyl-2β-carbomethoxy-3β-(4-iodophenyl)nortropane (123I-FP-CIT) SPECT quantitative methods in patients with neurodegenerative syndromes as referenced to neuropathologic findings. Methods:123I-FP-CIT-SPECT and neuropathologic findings among patients with neurodegenerative syndromes from the Mayo Alzheimer Disease Research Center and Mayo Clinic Study of Aging were examined. Three 123I-FP-CIT SPECT quantitative assessment methods-MIMneuro, DaTQUANT, and manual region-of-interest creation on a workstation-were compared with neuropathologic findings describing the presence or absence of Lewy body disease (LBD). Striatum-to-background ratios (SBRs) generated by DaTQUANT were compared with the calculated SBRs of the manual method and MIMneuro. The left and right SBRs for caudate, putamen, and striatum were evaluated with the manual method. For DaTQUANT and MIMneuro, the left, right, total, and average SBRs and z scores for whole striatum, caudate, putamen, anterior putamen, and posterior putamen were calculated. Results: The cohort included 24 patients (20 [83%] male, mean age for all patients at death, 75.4 ± 10.0 y). The antemortem clinical diagnoses were Alzheimer disease dementia (n = 6), probable dementia with Lewy bodies (n = 12), mixed Alzheimer disease dementia and probable dementia with Lewy bodies (n = 1), Parkinson disease with mild cognitive impairment (n = 2), corticobasal syndrome (n = 1), idiopathic rapid-eye-movement sleep behavior disorder (n = 1), and behavioral-variant frontotemporal dementia (n = 1). Seventeen (71%) had LBD. All 3 123I-FP-CIT SPECT quantitative methods had an area under the receiver-operating-characteristics curve ranging from more than 0.93 to up to 1.000 (P < 0.001) and showed excellent discrimination between LBD and non-LBD patients in each region assessed (P < 0.001). There was no significant difference between the accuracy of the regions in discriminating the 2 groups, with good discrimination for both caudate and putamen. Conclusion: All 3 123I-FP-CIT SPECT quantitative methods showed excellent discrimination between LBD and non-LBD patients in each region assessed, using both SBRs and z scores.
Keywords: 123I-FP-CIT SPECT; 123I-ioflupane; Lewy body disease; dementia with Lewy bodies; neuropathology.
© 2020 by the Society of Nuclear Medicine and Molecular Imaging.
Figures
Similar articles
-
The value of multimodal imaging with 123I-FP-CIT SPECT in differential diagnosis of dementia with Lewy bodies and Alzheimer's disease dementia.Neurobiol Aging. 2021 Mar;99:11-18. doi: 10.1016/j.neurobiolaging.2020.12.009. Epub 2020 Dec 15. Neurobiol Aging. 2021. PMID: 33422890 Free PMC article.
-
Dopamine transporter imaging for the diagnosis of dementia with Lewy bodies.Cochrane Database Syst Rev. 2015 Jan 30;1(1):CD010633. doi: 10.1002/14651858.CD010633.pub2. Cochrane Database Syst Rev. 2015. PMID: 25632881 Free PMC article.
-
The diagnostic performance of functional dopaminergic scintigraphic imaging in the diagnosis of dementia with Lewy bodies: an updated systematic review.Eur J Nucl Med Mol Imaging. 2023 Jun;50(7):1988-2035. doi: 10.1007/s00259-023-06154-y. Epub 2023 Mar 15. Eur J Nucl Med Mol Imaging. 2023. PMID: 36920494 Free PMC article.
-
Diagnostic Value of Swallow Tail Sign at Brain MRI in Patients with Clinically Uncertain Parkinsonian Syndrome.Radiology. 2025 Jul;316(1):e240680. doi: 10.1148/radiol.240680. Radiology. 2025. PMID: 40626875
-
A Head-to-Head Comparison of 18 F-FP-CIT and 18 F-FDOPA PET/CT in Early Parkinson Disease.Clin Nucl Med. 2025 Sep 1;50(9):809-816. doi: 10.1097/RLU.0000000000006024. Epub 2025 Jul 1. Clin Nucl Med. 2025. PMID: 40601476 Free PMC article.
Cited by
-
Marked Decreased Tracer Binding in 123 I-FP-CIT SPECT Scans From Lisdexafetamine Dismesylate Interaction: A Case Report.Clin Neuropharmacol. 2024 Jan-Feb 01;47(1):26-28. doi: 10.1097/WNF.0000000000000579. Epub 2024 Feb 2. Clin Neuropharmacol. 2024. PMID: 38193851 Free PMC article.
-
Brain glucose metabolism and nigrostriatal degeneration in isolated rapid eye movement sleep behaviour disorder.Brain Commun. 2023 Feb 2;5(1):fcad021. doi: 10.1093/braincomms/fcad021. eCollection 2023. Brain Commun. 2023. PMID: 36844148 Free PMC article.
-
Dopaminergic imaging and clinical predictors for phenoconversion of REM sleep behaviour disorder.Brain. 2021 Feb 12;144(1):278-287. doi: 10.1093/brain/awaa365. Brain. 2021. PMID: 33348363 Free PMC article.
-
Research diagnostic criteria for mild cognitive impairment with Lewy bodies: A systematic review and meta-analysis.Alzheimers Dement. 2023 Jul;19(7):3186-3202. doi: 10.1002/alz.13105. Epub 2023 Apr 24. Alzheimers Dement. 2023. PMID: 37096339 Free PMC article.
-
The value of multimodal imaging with 123I-FP-CIT SPECT in differential diagnosis of dementia with Lewy bodies and Alzheimer's disease dementia.Neurobiol Aging. 2021 Mar;99:11-18. doi: 10.1016/j.neurobiolaging.2020.12.009. Epub 2020 Dec 15. Neurobiol Aging. 2021. PMID: 33422890 Free PMC article.
References
-
- Williams MM, Xiong CJ, Morris JC, Galvin JE. Survival and mortality differences between dementia with Lewy bodies vs Alzheimer disease. Neurology. 2006;67:1935–1941. - PubMed
-
- Boström F, Jonsson L, Minthon L, Londos E. Patients with Lewy body dementia use more resources than those with Alzheimer’s disease. Int J Geriatr Psychiatry. 2007;22:713–719. - PubMed
-
- McKeith I, O’Brien JT, Walker Z, et al. . Sensitivity and specificity of dopamine transporter imaging with 123I-FP-CIT-SPECT in dementia with Lewy bodies: a phase III, multicentre study. Lancet Neurol. 2007;6:305–313. - PubMed